
As Approval of Medical Cannabis Spreads State by State, Product Labeling Improvements Are a Must
Problem: Anecdotal support, public opinion, and state laws in the US are outpacing scientific research involving medical marijuana, more professionally known as medical cannabis. Medical cannabis differs from the street product in that the plant must be reliably grown and handled in a manner that resembles good manufacturing practices. This allows growers to assay and establish the products’ contents with the intent of passing that information on to dispensaries and patients. However, lack of federal regulation has allowed for heterogeneity of state programs, yielding a wide variety of cannabis formulations, products, flashy strain names, and patient safety concerns.
For example, the use of strain (or brand) names is prevalent, but studies have shown that there are genetic inconsistencies among products with the same strain name.1-4 Furthermore, the lack of consistency in state cannabis labeling requirements, along with the lack of involvement of healthcare professionals, has given rise to labeling practices that risk patient safety. Thus, it is difficult for dispensaries to provide patients with products that are clearly labeled, which is a critical component for safe and reproducible effects.
Components of Medical Cannabis
Cannabis sativa has many phenotypes (strains) that include hundreds of chemicals (cannabinoids) produced in varying amounts based on the strain and growing conditions. As a comparison, think of all the varieties and tastes of apples, including regional varieties, crab apples, and genetic hybrids such as “grape-apples.” The two most notable cannabinoids are tetrahydrocannabinol (THC) and cannabidiol (CBD), although cannabis has many other physiologically active molecules whose effects are not fully understood.
THC is associated with psychoactivity (or psychotoxicity), including euphoria, relaxation, pain relief, anxiety, and memory impairment. The psychoactive effects tend to be dose limiting, and taking too much can make patients feel uncomfortable. When talking to patients, it is helpful to describe the psychoactive effects as impairment or intoxication and to caution that it might cause light-headedness and postural hypotension, increasing the risk of falls. THC has been associated with cannabis use disorder, while CBD has not.
CBD is not psychoactive, and preclinical data suggests it has anti-inflammatory, analgesic, anti-nausea, antiemetic, antipsychotic, anxiolytic, and antiepileptic properties. Patients may take escalating doses of CBD because they do not feel any cognitive impairment. Common side effects include headache, diarrhea, restlessness, and/or somnolence.
Both THC and CBD may interact with other medications. Examples include interactions with epilepsy medications and warfarin. While the dose of THC is directly correlated with cognitive and motor function effects, the dose of CBD may be more predictive of the magnitude of possible drug interactions.
Dosage Forms
There are a variety of medical cannabis dosage forms, producing different pharmacokinetic and pharmacodynamic effects. Common formulations include capsules and liquids for oral use, vaporized products (extracts and raw flower), sublingual drops, transmucosal adhesives, topical creams/ointments, transdermal patches, and suppositories.
Nonstandard, Confusing Labeling
All state laws require products to be assayed and labeled by the grower, and ideally verified by an accredited third-party lab, for at least the two major cannabinoids currently of interest, THC and CBD. While the total cannabinoid content must be listed on the label, only THC and CBD individual quantities must be expressed on the label. The amounts of these two cannabinoids are clinically relevant for managing patients’ symptoms. However, the way these components are expressed on labels is not standardized (Figure 1) and can lead to errors.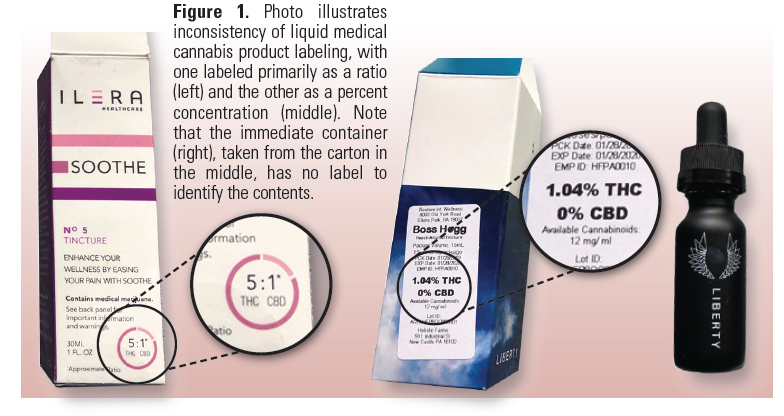
Ratio expressions. The two primary cannabinoids are often expressed as a ratio of either THC:CBD or CBD:THC. So, the first problem is that no international or national standard exists governing which cannabinoid is listed first when presented as a ratio, and most state regulations do not dictate a formal convention. The order of components in the ratio may differ between growers and even within a grower’s product line, causing confusion when determining which product to use. Look-alike product labeling (Figure 2), particularly within a grower’s product line, has also been reported, leading to confusion between products containing different ratios of THC and CBD.

Percent concentrations. In addition to (or in place of) ratio expressions, some products are labeled with the percent concentration. This makes it difficult for staff in dispensaries and patients to calculate the amount of THC and/or CBD in the product. For example, would you be able to easily identify the amount of THC and/or CBD in 0.5 mL of a 0.037% product, especially if the mg/mL amount is not clearly listed? With some products, the mg amount of each primary ingredient can be found on container labels, which is preferred for dosing and consistency but could still cause confusion in patients who are more familiar with ratio expressions. It is critical to know the actual mg amount of each primary component, especially THC, which is most likely to elicit clinical and/or adverse effects. But too often, the mg amount of a liquid product is listed without a corresponding volume, preventing the ability to determine the concentration. And again, there is no standard. The Sidebar (right column) provides an example of this problem along with several other labeling issues.
Labeling of the immediate container. For some liquid products and almost all vaporization cartridges, only the outer carton is labeled, and the immediate container (bottle or cartridge) is not labeled at all (Figure 1). If the carton is discarded or lost, the unlabeled product may be confused with something else.
Label contents. Certain dosage forms also lack important ingredient and label information. For example, the labeling of tinctures does not always include the alcohol content, and frequently the term tincture is misapplied to products that do not contain alcohol. Transdermal patches often do not include key information such as onset and duration of effect, delivered dose, and cautions about possible systemic effects. It should also be mentioned that there are terpenes present in essential oils of the marijuana plant that give it its fragrance, which are also physiologically active molecules that have been known to have clinical effects—from anxiolytic to anti-inflammatory effects, and more.5 Product assays will sometimes list plant terpenes, but not all states require this.
Safe Practice Recommendations: To promote patient safety, labeling standards are needed for medical cannabis products, at the very least to specify THC and CBD contents and concentrations accurately in metric units, and healthcare providers need to know how to interpret the label information. Because ratio expressions are predominantly used today, medical cannabis products must conform to some type of labeling convention to signify whether THC or CBD is listed first in a ratio expression. However, we are not convinced that ratio expressions should be used at all given the potential for errors as seen with other medications previously expressed this way (e.g., EPINEPHrine 1:10,000), which is now prohibited on most medication labels.
The common practice of expressing concentrations as percentages, without a total volume or the mg amount per mL, introduces significant risk of error when calculating the dose, especially one based on a nonstandard serving size. Clearly mandating the expression of strengths and concentrations of the THC and CBD contents in metric units (e.g., mg, g, mg/mL) would provide the safest communication to both patients and healthcare providers. Additionally, all immediate product containers should be labeled, not just the outer packaging.
Ensuring that all inactive ingredients, especially additives, in a product are included in the labeling is critical to mitigate allergic reactions to dyes and flavoring agents. Drug-drug binding interactions can result from the product’s vehicle (e.g., sesame oil) and other herbal products (e.g., melatonin) that are sometimes added. This information could be provided on a side panel to avoid clutter on the primary display panel.
The US Food and Drug Administration (FDA) approved a single cannabidiol product, EPIDIOLEX (Greenwich Biosciences) in June 2018 for the treatment of seizures associated with Lennox-Gastaut and Dravet syndromes in patients age 2 and older. It is available by prescription only. However, for all other forms of medical cannabis, healthcare providers interacting with patients should clearly communicate that these products are not approved by FDA for any medical conditions; thus, therapy is considered investigational, and safety, including reproducibility of response between products, is not fully understood. Further, CBD-only products that are routinely sold on the internet and in retail establishments have not been evaluated by FDA for potency, purity, or safety. There are many reports of CBD-only products containing either no detectable CBD, or significantly more CBD than is on the label. Based on studies, approximately 1 in 5 CBD-only products contains detectable amounts of THC, putting patients unknowingly at risk of impairment as well as testing positive on urine drug screens for THC.6,7
ISMP and FDA would like to learn more about labeling and packaging problems or other practice issues with medical cannabis. Please report all hazards, close calls, and errors with medical cannabis to the ISMP National Medication Errors Reporting Program (ISMP MERP), and ISMP will forward the reports to FDA. Look for more about medication safety issues with medical cannabis (e.g., duplicate therapy, drug interaction checking, managing hospitalized patients who use medical cannabis at home) in subsequent newsletters throughout the year.
ISMP thanks Christine Roussel, PharmD, BCOP, Director of Pharmacy at Doylestown Hospital in PA, for providing this article.
References
-
Schwabe AL, McGlaughlin ME. Genetic tools weed out misconceptions of strain reliability in Cannabis sativa: implications for a budding industry. bioRxiv. May 28, 2018.
-
National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press; 2017. https://doi.org/10.17226/24625
-
World Health Organization (WHO). Cannabidiol (CBD) critical review report. 2018. Prepared for participants of the 40th Expert Committee on Drug Dependence, Geneva, June 4-7, 2018.
-
Health Canada. Information for health care professionals: cannabis (marihuana, marijuana) and the cannabinoids. October 2018.
-
Nuutinen T. Medicinal properties of terpenes found in Cannabis sativa and Humulus lupulus. Eur J Med Chem. 2018;157:198-228.
-
Bonn-Miller MO, Loflin MJE, Thomas BF, Marcu JP, Hyke T, Vandrey R. Labeling accuracy of cannabidiol extracts sold online. JAMA. 2017;318(17):1708-9.
-
US Food and Drug Administration (FDA). Warning letters and test results for cannabidiol-related products. April 2, 2019.