
CMS 30-minute Rule for Drug Administration Needs Revision
In our June 17, 2010 newsletter, we covered a precarious topic best known as the “30-minute rule”—a requirement in the Centers for Medicare & Medicaid Services (CMS) Conditions of Participation Interpretive Guidelines to administer scheduled medications within 30 minutes before or after the scheduled time. In our July 2010 nursing newsletter, Nurse Advise-ERR, we asked frontline nurses who are most directly affected by the 30-minute rule to weigh in on the issue by completing a short survey. And WOW, did they ever! More than 17,500 nurses responded to our survey, providing more than 8,000 additional comments (see Table 1), making it very clear that the issue is of great significance to nurses.
|
Comments About At-Risk Behaviors
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Comments About Associated Errors/Harm
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
General Comments
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Respondent profile and compliance rates
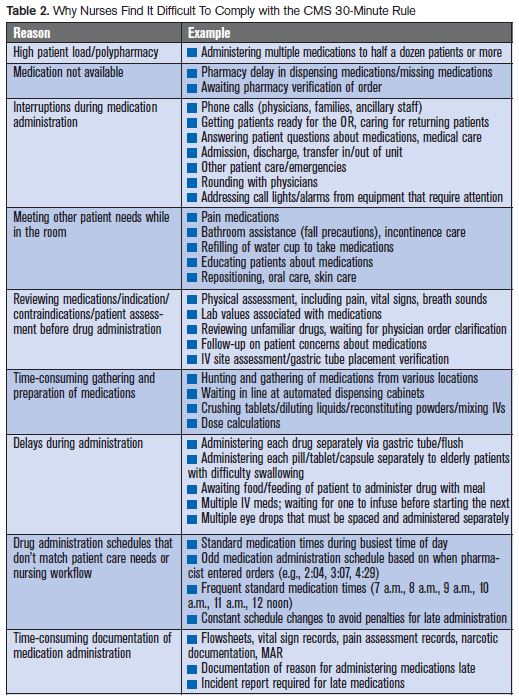
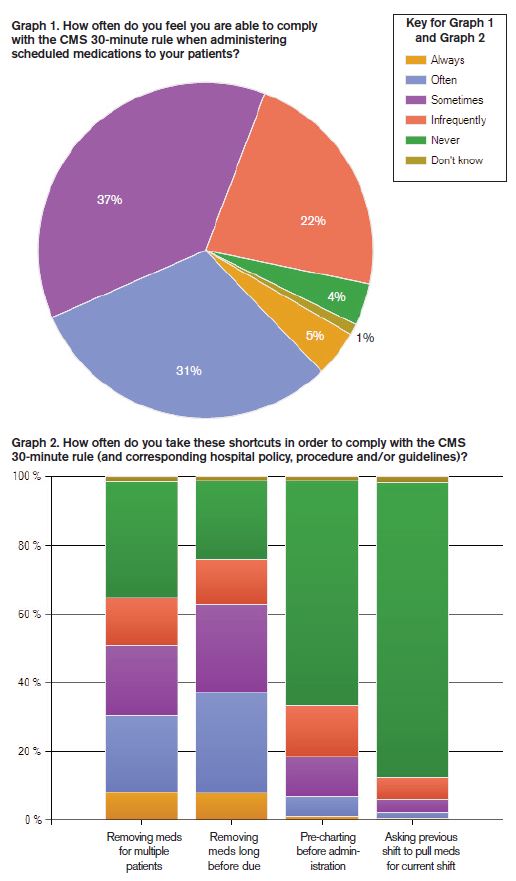
Almost half of the responding nurses work on medical/surgical units, and the other half work in critical care, telemetry, or specialty inpatient units. Most nurses feel that the 30-minute rule is unsafe, unrealistic, impractical, and virtually impossible to follow. Approximately three out of four respondents (70%) told us their organization enforces such a policy. Of these nurses, only five of every 100 (5%) were always able to comply with the policy, while more than half (59%) were infrequently or only sometimes compliant (see Graph 1). Why nurses find it difficult to comply with the 30-minute rule was expressed by many (see Table 2), including a nurse who sent a pragmatic yet eloquent account of a Day in the Life of a Nurse (see Sidebar that follows this article).
A new pressure to comply
The advent of electronic medication administration records (eMARs) has brought about additional pressure for nurses to administer medications within a required timeframe, as this technology can now easily detect and quantify all late drug administration if used as intended. On a paper MAR, nurses reported that they often just initial the medication entry or document the drug as being administered at the scheduled time, not the actual time; thus, “late” administration was not clearly identifiable. With eMARs, nurses receive visible cues—often the angst-provoking “red font” of a medication entry—if the drug has not been administered on time. Furthermore, bar-coding systems can track and report all late drug administration and link each occurrence to an individual nurse, which often requires an incident report and can lead to unwarranted disciplinary action. To avoid disciplinary action, many honest nurses admitted to documentation of drug administration at the scheduled time, not the actual time. Even the computer can be tricked.
At-risk behaviors (shortcuts)
Many nurses commented that they felt the 30-minute rule set them up to fail by compelling them to take shortcuts to administer medications within the required time and pressuring them to perform like “med-pusher” robots rather than well-trained healthcare professionals who engage in critical thinking.
Among the at-risk behaviors presented in the survey (see Graph 2), removing medications from automated dispensing cabinets (ADCs) or other storage locations well before administration time, and gathering more than one patient’s medications at a time, were the most common shortcuts nurses took to comply with the 30-minute rule. Approximately 1 of every 10 respondents always takes these shortcuts, and 1 in 4 often takes these shortcuts. While nurses reported that technology such as ADCs has made medication administration safer, it has also slowed the process—standing in line, for instance, to obtain medications from ADCs. Thus, to comply with the 30-minute rule, nurses told us they often feel compelled to take shortcuts during medication administration.
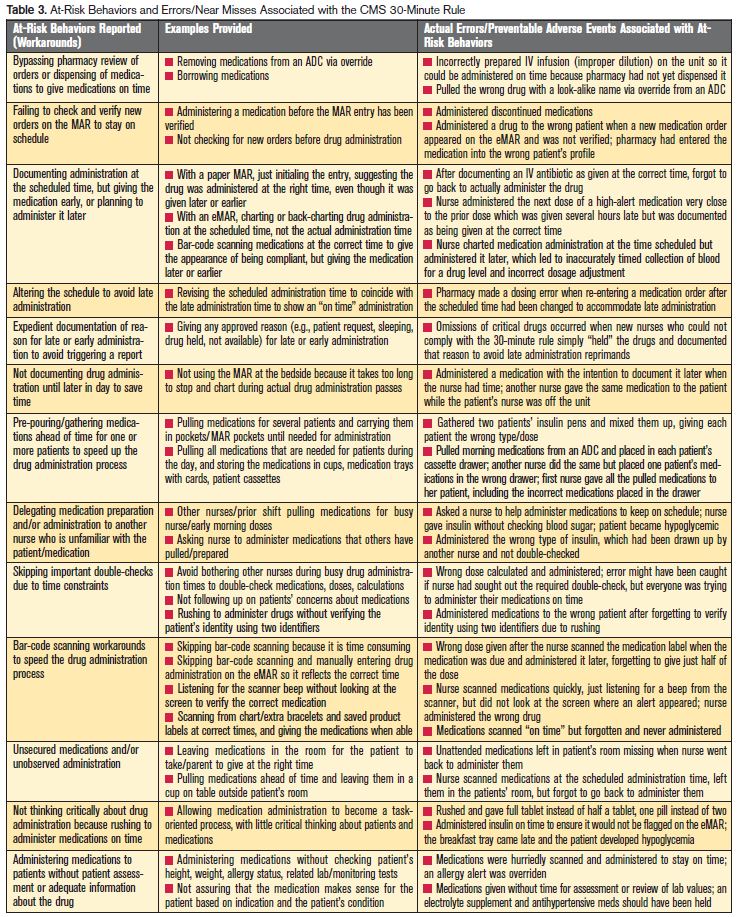
About one-third of nurses reported documenting medication administration at the scheduled time and administering the medications earlier or later. About 15% also reported asking coworkers from a previous shift to prepare their patients’ medications for administration during the first few hours of their shift. Nurses provided perceptive details regarding additional at-risks behaviors (see Table 3) they engaged in to comply with the 30-minute rule, including:
- Bypassing pharmacy review of orders and borrowing medications or preparing IV solutions on the unit to facilitate on-time medication administration
- Administering medications before conducting a physical assessment of the patient and/or checking vital signs, lab values, weight, and allergy status
- Rushing to administer a new medication before the MAR entry has been verified
- Altering the drug administration schedule to the time the drug was actually administered to avoid late administration
- Providing any approved reason for late administration (e.g., patient request) regardless of accuracy
- Not documenting drug administration until later in the day to save time
- Skipping important double-checks to save time during drug administration
- Skipping bar-code scanning because it is time consuming and results in documentation of late drug administration
- Scanning medications at the correct time using the patients’ charts/extra identification bracelets, locking the drugs in a cabinet, and dispensing them when able
- Leaving medications in the patient’s room and asking patients to take them as soon as possible
- Allowing medication administration to become a task-oriented process, with little critical thinking about whether the drug is indicated for the patient or the order for the drug is accurate and safe.
Not unexpected, but nevertheless alarming, one in four nurses (25%) reported making and/or observing medication errors in which attempts to comply with the 30-minute rule played a large role. Considering that a small percent of errors are recognized, detected, or reported in most organizations, the actual error rate associated with the 30-minute rule may be much higher. The most common types of errors reported by nurses include:
- Administering a discontinued medication, a whole tablet instead of half a tablet, one tablet instead of two tablets, or an entire ampul/vial of medication instead of a partial dose because the medications were pulled early and the patient’s chart and/or MAR were not referenced for verification prior to administration
- Administering medications to the wrong patient because multiple patients’ medications were gathered at the same time
- Omitting doses after pulling medications and/or documenting medication administration ahead of time and then forgetting to administer the drugs
- Administering duplicate doses because the nurse administering the first dose did not take the time to document administration until later in the day
- Calculating doses incorrectly and administering wrong doses because they are focused on administering medications on time and did not seek out another nurse to double-check the math
- Preparing IV solutions incorrectly on nursing units instead of waiting for pharmacy to prepare and dispense them so that the solution can be started within the allotted time
- Administering IV medications more rapidly than recommended to administer all IV medications within the allotted time.
Table 3 provides many more examples of errors reported by the nurses along with the at-risk behaviors that contributed to each.
Other concerns about the rule
More than 3,000 nurses (approximately 20% of all respondents) said they were aware that their organization had encountered Joint Commission or state surveyors within the past 5 years who required strict adherence to the CMS 30-minute rule. Although nurses have long been taught to give medications in a timely manner, many expressed anger toward CMS for the 30-minute rule in the Interpretive Guidelines; a few even questioned whether the rule was evidence-based. Nurses overwhelmingly stated that the rule was exposing patients to unsafe conditions and neglectful situations, particularly if nurses felt they did not have the time to assess patients before drug administration and prioritize their work based on patient needs rather than adhering to the rule. Numerous nursing instructors also commented that the 30-minute rule makes it difficult to teach students safe practice habits because the rule places undue priority on the timeliness of medication administration and not enough on safety.
As a last example, many nurses reported that attempts to meet the 30-minute rule interfered with their ability to be respectful of patients. For example, nurses felt pressured to administer medications to patients even if they were in the bathroom, getting bathed, or using a bedpan or bedside commode, just to ensure timely medication administration, which is often not necessary from a clinical perspective. Nurses also reported that patients feel rushed and unimportant when nurses hurry out of the room to administer medications to the next patient. Oftentimes, nurses cannot take the time to educate patients about their medications, and patients’ questions go unasked and unanswered, particularly when they perceive the nurse’s hectic pace and don’t feel permitted to ask questions.
Changing the rule
The vast majority—up to 9 out of 10 nurses—who participated in our survey believe the 30-minute rule should be changed, with most (75%) opting for 60-minutes before or after the scheduled time for medications administered every 4 hours or less often. Approximately 1 in 5 nurses (20%) thought the 60-minute timeframe should be accompanied by more specific timeframes for certain drugs (e.g., antibiotic, insulin, antihypertensive), and another 22% suggested this option alone. Comments from nurses overwhelmingly suggest that they should be able to exercise clinical judgment and critical thinking to make exceptions to any rule when necessary—something many do not feel empowered to do with the seemingly sole emphasis on timeliness. Around 6% of nurses felt there should be no timeframe dictated. Many nurses commented that unsafe staffing levels make it impossible to comply with the 30-minute rule and suggest that compliance will only be possible if staffing and work conditions are improved.
Next steps
Our survey has proved to be an excellent way to gain insight and convey the nurses’ point of view about the 30-minute rule. ISMP has already initiated conversation with CMS staff and provided them with preliminary findings from the survey. As a result, we are happy to report that CMS staff has been receptive to the findings and agreed to take them under advisement. Based in large part on the findings from this survey, ISMP is currently working with an expert advisory group to document what we believe would represent best practices associated with timely administration of medications. We plan to publish our recommendations in this newsletter in the very near future. We thank the many thousands of nurses who took time to respond to our survey and provide comments. We can assure all responding nurses that their voices have been heard!
Sidebar: A Day in the Life of a Nurse
You asked how does strict adherence to the 30-minute rule create an opportunity for error? As a bedside nurse, I can tell you first-hand. But first, let me give you a little peek into what medication administration looks like on my unit.
First, many patients come into the hospital on multiple medications from home, meaning that it is not unrealistic to be administering 5-10 chronic medications per patient (in addition to administering pain medication, antibiotics, managing IV lines, etc.) during my 0900 medication pass time.
Second, medication administration does not happen in isolation of all other responsibilities and demands for my attention, despite efforts to minimize and eliminate interruptions during medication pass times. On a typical day shift, I have four patients. Many times I must wait in line for access to one of two automated dispensing cabinets (we are a 36-bed unit), especially during 0900 medication pass times. Then I must safely take out each medication while double-checking it against the electronic medication administration record (eMAR) for that patient. After that, I must find any medication that is not stocked in the automated dispensing cabinet (ADC). This can be in any one of four locations: 1) the patient’s individual medication cassette, 2) the refrigerator, 3) the other ADC, or 4) in the pharmacy (e.g., a missing medication). I have to prepare a label for any medications that I need to draw up into a syringe. For IV piggyback medications, I must first mix them and then prepare a label.
Next, I travel down the hall with my eMAR and all the medications. Hopefully, when I arrive in the room, the patient is ready for me, water cup in hand, for her medications. I check the eMAR against the patient’s armband and individually open each little packet of unit-dose medication, while explaining to the patient the medication, dosage, purpose, etc., and answer any concerns or questions. (I tease my patients that some of those little packets are “nurse-proof”—they can be so cumbersome to open.) Hopefully, I make it from the counter-top, where I opened all the medications successfully, to the patient without dropping anything or knocking over the cup. Then I watch as my 83-year-old patient takes ONE pill at a time, as I cautiously survey her every attempt to reach her mouth, so as to catch any medications that may fall out of her hand/cup and into the bed sheets or down her gown. Then I stop and take her blood pressure before she takes her antihypertensive medications. Finally, I go back to my eMAR and document with my initials every medication I administered...and the TIME. On to the next patient, right? Oh, no—the first patient needs to use the bathroom (a 20-minute activity, as she is an elderly post-operative patient with a knee replacement, and I need to help her get up to use the bedside commode). But then again, that gives me the opportunity to assess the patient’s strength and ability to follow commands, to scan and assess her skin, etc. I hope you are getting the idea that medication passes are time consuming, and that patients have other needs that I cannot ignore. I just gave you one very common scenario. Many more opportunities for distraction and interruptions occur that cause medication administration times to be delayed.
So where’s the opportunity for error? The frustration at the whole process of medication administration causes distraction, one of the most frequent contributors to medication administration errors. The time crunch to administer medications within the 30-minute rule causes nurses to find workarounds...like pilfering another patient’s cassette for a missing medication, documenting that the nurse gave a medication at 0900 (to keep in compliance and not get “caught” on audit) when it was really given at 1005, or withdrawing and preparing two different patients’ medications at the same time to save time. Both patients are in a semi-private room…why walk down the hall, back and forth, twice? Just bring both patient’s meds to the room at the same time! These are just some examples of a nurse’s effort to “be in compliance” rather than do what is in the best interest of safety for the patient.
Giving nurses more flexibility for some medications and administration times, and educating us as to how/why these workarounds put our patients and our practice at risk is the answer. I hope this gives you some insight into the challenges of meeting the 30-minute rule.
Editor’s note:This bedside nurse’s commentary also gives insight into why physicians, pharmacists, and hospital leaders need to assist nurses in making medication administration as efficient and safe as possible (e.g., dispense liquids not tablets that need crushing for tube-fed patients, dispense unit dose syringes in the exact dose, provide on-time drug delivery, provide easy access to drug information). Still aren’t convinced? Take some time to walk alongside a nurse one day. We’re sure you’d be warmly welcomed.