
Guidelines for Timely Medication Administration: Response to the CMS "30-minute rule"
In our September 9, 2010 newsletter, we discussed the results of our survey regarding the requirement in the Centers for Medicare & Medicaid Services (CMS) Conditions of Participation Interpretive Guidelines to administer medications within 30 minutes before or after the scheduled time. The survey elicited responses from almost 18,000 nurses. Respondents made it clear that changes to drug delivery methods and gradual increases in the complexity of care, number of prescribed medications per patient, and number of patients assigned to each nurse have made the long-standing CMS “30-minute rule” troublesome. Many nurses now feel the rule is unsafe, impossible to follow, and often unnecessary from a clinical perspective. Aware that nurses were struggling to comply with the rule and that surveyors were sometimes citing hospitals for noncompliance, we conducted the survey to prepare for interaction with CMS leaders to discuss our concerns regarding the rule’s unintended effects on patient safety. Preliminary interaction has taken place, and CMS has indicated openness to suggestions for improvement.
Nurses who responded to our survey reported feeling pressured to take these and other shortcuts to comply with the CMS 30-minute rule:
- Preparing IV solutions on the unit, thus bypassing pharmacy verification and specialized aseptic techniques
- Administering medications before conducting a physical assessment of the patient and/or checking vital signs, lab values, weight, and allergy status
- Removing medications from automated dispensing cabinets (ADCs) via override without a pharmacist’s safety review
- Borrowing medications from one patient to administer to another patient
- Not thinking critically about drug administration while rushing through verification of new orders and actual drug administration
- Documenting administration at the scheduled time, but actually giving the drug early or late
- Altering drug administration schedules to avoid documenting late administration
- “Pre-pouring” medications ahead of time for one or more patients to accelerate the drug administration process
- Skipping important double-checks due to time constraints
- Failing to use barcode scanning to avoid documentation of late administration
- Leaving medications in the room for the patient to take at the right time.
The above and other at-risk behaviors—which are unintended consequences of attempts to comply with the CMS 30-minute rule—have led to errors, some harmful. On the other hand, for some critical patient populations, certain first doses, and time-critical scheduled medications (e.g., rapid-acting insulin), delays in administration can result in harm. Therein lies the dilemma faced by nurses and pharmacists responsible for dispensing and administering medications in a timely—and also safe—manner. A one-size-fits-all, inflexible requirement to administer all scheduled medications within 30 minutes before or after their scheduled times is a precarious mandate since relatively few medications truly require exact timing of doses; thus, the rule is ill-suited for the vast majority of medications that are not time critical. A rigid, standard requirement also does not encourage or allow healthcare professionals to utilize critical thinking to prioritize patient care appropriately or to manage the unexpected, which is commonplace in healthcare. In a setting of competing priorities, administration of non-time-critical medications may appropriately be lower on the list of priorities relative to other more crucial time-sensitive clinical tasks.
Since publication of the survey results, ISMP has been working towards documenting what we believe would represent best practices associated with timely administration of scheduled medications. Scheduled medications include all maintenance doses administered according to a standard, repeated cycle of frequency (e.g., q4h, QID, TID, BID, daily, weekly, monthly, annually). For the purpose of ISMP’s guidelines that follow, scheduled medications DO NOT include:
- STAT and Now doses
- First doses and loading doses
- One-time doses
- Specifically timed doses (e.g., antibiotic for surgical patient 10 minutes before incision, drug desensitization protocols)
- On-call doses (e.g., pre-procedure sedation)
- Time-sequenced or concomitant medications (e.g., chemotherapy and rescue agents, n-acetylcysteine and iodinated contrast media)
- Drugs administered at specific times to ensure accurate peak/trough/serum drug levels
- Investigational drugs in clinical trials
- PRN medications.
The following Guidelines for Timely Administration of Medications (summary in Table 1) represent a synthesis of ISMP expertise, review of available literature on the risks associated with early and delayed administration of maintenance drug therapy, and advice from survey participants and an expert clinical advisory group of more than 20 clinicians—many of whom are currently practicing in healthcare settings. The guidelines may seem detailed; however, timely medication administration is a multifaceted issue that cannot be managed appropriately with a single standard. We welcome your comments on these guidelines ([email protected]) by February 15, 2011. We will then post a final position statement on timely drug administration on our website. We also plan to interact with CMS to discuss possible alterations in the CMS guidelines to best facilitate both timely and safe drug administration.
We have also provided Supporting Guidelines (Table 2) to assist hospitals in meeting the proposed Guidelines for Timely Administration of Medications.
Guidelines for Timely Administration of Medications
1. Identify a hospital-specific list of time-critical scheduled medications.1 Time-critical scheduled medications are those where early or delayed administration of maintenance doses of greater than 30 minutes may cause harm or result in substantial sub-optimal therapy or pharmacological effect. While the list of time-critical scheduled medications will include a limited number of drugs, a universal list is not desirable because hospitals that treat different patient populations (e.g., mental health, oncology, transplant patients, pediatrics, premature infants) may need to include different medications to address respective risks.1 Similarly, some hospitals that serve very diverse patient populations may decide to identify both hospital-wide and unit-specific time-critical medications.
Examples of time-critical scheduled medications include:
- Immunosuppressive agents used for the prevention of solid-organ transplant rejection or to treat myasthenia gravis
- Certain drugs that require administration within a specified short period of time before, after, or with meals—for example, rapid-, short-, or ultra-short-acting insulins, certain oral antidiabetic agents (e.g., acarbose, nateglinide, repaglinide, glimepiride), alendronate, and pancrelipase.
Additionally, because some scheduled medications can be time-critical for certain patients given their diagnoses (e.g., scheduled parenteral anti-infective agents for a patient with worsening sepsis), the list may include some drugs that are time-critical only when used for a specific diagnosis or indication. Further, policies should allow prescribers, pharmacists, or nurses to declare any medication to be time-critical (i.e., must be given within 30 minutes before or after the scheduled time) by including this designation with the medication order and/or medication administration record (MAR) entry.
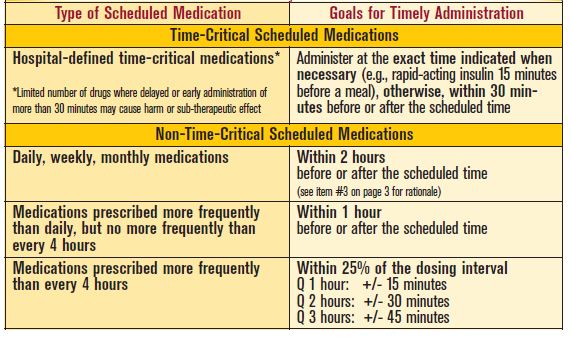
2. Establish guidelines that facilitate pharmacy order review, dispensing, and nurse administration of the hospital-identified, time-critical scheduled medications within 30 minutes before or 30 minutes after the scheduled time (or more exact timing when indicated, as with rapid-, short-, and ultra-short-acting insulins). MAR entries for hospital-identified time-critical scheduled medications should be clearly designated to remind staff that these drugs require meticulous attention to timely administration (e.g., administered at the designated time, or plus or minus 30 minutes from the scheduled time, if appropriate).
3. Establish guidelines for timely drug administration of scheduled non-time-critical medications as follows:
- Daily, weekly, or monthly medications: Administer these medications plus or minus 2 hours from the scheduled time. (Although it is generally safe to administer daily/weekly/monthly medications within a timeframe that exceeds 2 hours, ISMP recommends keeping the timeframe to 2 hours before or after the scheduled time to prevent accidental omission of doses that might be more easily forgotten if delayed more than 2 hours.)
- Medications administered more frequently than daily but not more frequently than every 4 hours (e.g., BID, TID, q4h, q6h): Administer these medications plus or minus 1 hour from the scheduled time.
- Medications administered more frequently than every 4 hours (e.g., q1h, q2h, q3h): Administer these medications within 25% of the dosing interval (e.g., plus or minus 15 minutes for hourly doses, plus or minus 30 minutes for every 2 hours dosing, plus or minus 45 minutes for every 3 hours dosing).
As an alternative to the guidelines in item #3, hospitals with electronic MARs (eMARs) may choose to establish a standard allowable percent of difference between the scheduled time and administration time—not to exceed 25%—for all non-time-critical medications if the eMARs can alert nurses in advance to an impending late dose and the allowable timeframe for administration.
4. Although not associated with the timing of scheduled medications, hospitals should also define targeted timeframes for administering first doses and loading doses of key medications, such as IV anti-infective agents, IV anticoagulants, and IV anti-epileptic medications where timeliness is critical (e.g., an emergency department patient with suspected sepsis should not wait several hours for administration of a prescribed anti-infective). Where electronic prescribing systems are available, the prescriber can also be queried regarding when the first dose should be administered given the standard administration times. While timely administration of first or loading doses of these drugs may be critical, many are not necessarily time-critical when it comes to subsequent maintenance doses. The targeted timeframes for first or loading doses of medications should be accompanied by procedures that facilitate achievement of the administration time goals.
| Topic | Description |
|---|---|
| Maintain adequate staffing levels | Maintain adequate staffing levels in the pharmacy and patient care units, based on workload and patient acuity, to facilitate timely order review, dispensing, drug administration, and patient monitoring. |
| Consider medication administration when making patient assignments | When planning nursing staff assignments for patient care, consider the following patient acuity factors: types of prescribed medications; quantity of time-critical medications; complexity of drug administration (e.g., preparing the drug, programming drug delivery devices, verification processes, administration procedures); total number of daily medications; frequency of drug administration; and the patient’s ability to swallow oral medications. |
| Use of automated dispensing cabinets (ADCs) | If using ADCs, ensure the number of cabinets on patient care units facilitates both safe (e.g., removal of one patient’s medications at a time) and timely (e.g., minimal waiting time to remove medications) drug administration. |
| Justification of early or late administration | Identify and clearly define justifiable reasons that time-critical and non-time-critical medications may be given early, delayed, or omitted (e.g., patient absence from unit, nausea/vomiting). |
| MAR documentation | Require staff who administer medications to document the exact time the drug was actually administered, rather than just initialing the MAR entry. If a medication was administered early, late, or has been omitted, require staff to document the reason. Ensure electronic and paper MARs provide sufficient space and prompts for this documentation. |
| Reference MARs | Require staff administering medications to always reference MARs that show times of the previously administered doses. This helps to avoid early administration of a dose that was previously administered late, resulting in a dosing interval that is too short (e.g., if a 9 a.m. dose of a maintenance opioid pain medication is given at 10 a.m., and the 1 p.m. dose is given at 12 p.m., the dosing interval is just 2 hours, thus risking over-sedation). |
| eMAR alerts | Define and configure (with vendor support as needed) eMAR alerts to show doses that will soon be overdue, that are beyond defined time limits or have been omitted, and to highlight previous doses that have been delayed/omitted. |
| Standard administration schedules |
Adhere to standard drug administration schedules based on the prescribed dosing frequency whenever possible. Exceptions to standard drug administration times may be appropriate for patients who self-administer chronic medications, to stagger numerous piggyback IV medications, or to keep a timecritical chronic medication on the same schedule used prior to admission. (While it may seem best to try to keep patients who take any type of chronic medication on the same administration schedule they were using at home, medication administration throughout the day during nonstandard times is prone to omissions; thus administration during standard times is recommended.) |
| Procedure to follow if medication administration is early or delayed |
Establish a procedure for clinical staff to follow if administration of a time-critical scheduled medication will be or has been delayed or administered early beyond allowable expectations.1 This procedure should include: 1) prescriber notification when an adverse outcome is anticipated or has occurred, 2) documentation in the patient’s chart and/or MAR regarding the reason administration of the dose was early or delayed, and 3) evaluation of the need to change the timing of future doses. |
| Event reporting | For learning purposes, require an event report for untimely administration of non-time-critical medications without a hospital-defined justifiable reason for the delay. Also require an event report for untimely administration of all time-critical medications, even if the reason for the delay was justifiable. Track untimely but justifiable administration of non-time-critical medications via end-of-shift reports or periodic aggregate data collection. |
| Data analysis | Review data from event reports, end-of-shift reports, and aggregate data collection to identify the causes of early or delayed drug administration, to revise the list of time-critical drugs as appropriate, and to make system-based changes to facilitate timely order review, dispensing, and administration of time-critical medications. Avoid punishment of individuals for late drug administration; instead, remedy the processes and environmental conditions that contributed to untimely administration. |
Reference:
1) National Patient Safety Agency (NPSA). Rapid response report NPSA/2010/RRR009: reducing harm from omitted and delayed medicines in hospital. February 2010.