
Part I: Survey Results Show Unsafe Practices Persist with IV Push Medications
In July and August 2018, we invited practitioners who administer intravenous (IV) push medications to adults to participate in a survey.1 The survey was conducted in response to three prior ISMP surveys that revealed numerous risky practices associated with the administration of IV push medications. These included the withdrawal of medications from prefilled syringes or cartridges, unnecessary dilution of IV push medications, and nurse preparation or manipulation of IV push medications at the bedside. Although the 2018 survey demonstrates a reduction in some of these unsafe practices, a surprising number of practitioners still report using prefilled syringes or cartridges as vials, diluting IV push medications despite their availability in a ready-to-administer form, unsafe labeling practices, and preparing IV medications at the bedside. Some of these unsafe practices appear to be associated with ongoing drug shortages, system vulnerabilities, and/or teaching strategies that perpetuate these practices.
Prior ISMP Surveys and Guidelines
In 2010, we conducted a survey on the impact of the economic crisis on medication safety, which uncovered long delays in dispensing pharmacy-prepared IV solutions and an increase in nurses preparing or manipulating parenteral medications on the clinical unit.2 In 2012, we conducted a survey to learn about practices when using CARPUJECT prefilled medication syringes, which exposed the widespread practice of using the cartridge as a vial to withdraw the medication into another syringe prior to administration.3 In 2014, we conducted a survey on IV push medications, which revealed unnecessary dilution associated with medications that were dispensed in ready-to-administer forms. The survey also uncovered the inappropriate use of prefilled normal saline flush syringes to dilute IV push medications, which results in mislabeled syringes.4
To address these safety concerns and others, ISMP held a national summit of expert stakeholders in 2014, which resulted in publication of the ISMP Safe Practice Guidelines for Adult IV Push Medications in 2015.5 Now, 3 years later, we have surveyed practitioners to understand current practices associated with IV push medications and to determine if ongoing drug shortages and teaching strategies around this critical skill have impacted current practices. In Part I, we present the findings from the latest survey. In Part II, which will appear in our next issue, we will provide recommendations for safe preparation and administration of adult IV push medications based on the survey results.
Respondent Profile
ISMP thanks the 977 practitioners who participated in our 2018 survey. Participants included nurses (93%), advance practice nurses (4%), and nurse anesthetists, anesthesiologists, and physicians (almost 3%). Most of the survey participants work in inpatient settings, including medical-surgical units (31%), critical care units (24%), surgical areas (13%), emergency departments (12%), labor and delivery units (7%), oncology units (3%), and a variety of other inpatient units (4%). Only 6% of the participants work in outpatient locations such as infusion centers, physician office practices, or diagnostic areas.
Ready-to-Administer Syringes
Only one-quarter (25%) of participants receive more than half of adult IV push medications in pharmacy-prepared or commercially available ready-to-administer syringes (Chart 1).
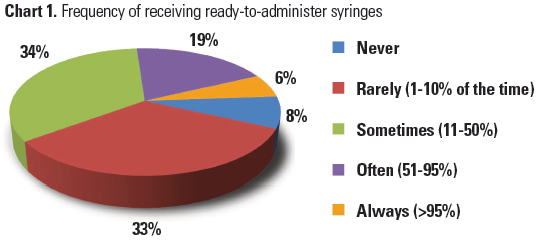
Just 6% always receive ready-to-administer syringes. Most participants (75%) receive half or fewer IV push medications in ready-to-administer syringes. Eight percent said they never receive ready-to-administer syringes—95% of these participants work in inpatient settings, mostly medical-surgical units. The medications most frequently NOT provided in ready-to-administer syringes include the following:
- Antiemetics (e.g., ondansetron, prochlorperazine, promethazine)
- Antipsychotics (e.g., haloperidol)
- Benzodiazepines (e.g., LORazepam, diazePAM)
- Antibiotics with short stability
- Opioids (e.g., fentaNYL, HYDROmorphone, morphine)
- Pantoprazole
- Metoprolol
- Furosemide
While many of these medications are marketed in a prefilled syringe, the syringes are, or have been, in short supply, making availability problematic.
Withdrawing Medications from a Prefilled Syringe and Transferring to Another
Two-thirds (66%) of participants reported withdrawing medications from a prefilled syringe (or cartridge) and transferring into another syringe to administer some or all of an IV push medication dose—16% do this more than half of the time they encounter a prefilled syringe. This may represent an increase from our 2012 survey, when 12% of respondents reported concern about this unsafe practice in the comments section of the survey. The most common reasons for withdrawing medication from a prefilled syringe are listed in Table 1, with dilution leading the way. Based on survey comments, other reasons for withdrawing medications from prefilled syringes are linked to drug shortages (e.g., to administer partial doses to promote opioid conservation), the need to filter some medications in cracked or particulate-containing prefilled syringes (www.ismp.org/ext/122), and the erroneous belief that a 10 mL syringe must be used to administer medications via an implanted port or peripherally inserted central catheter (PICC). (According to the Infusion Nurses Society, clinicians should use a syringe appropriately sized for the medication once patency has been confirmed using a 10 mL syringe.6)
| Reason | Percent of Respondents | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dilution | 64 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No designated syringe (cartridge) holder | 22 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Taught to do this | 15 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hard to read syringe dose increments | 14 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Syringe without a needleless connector or removable needle | 14 (e.g., opioids, insulin, heparin) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Other | 22 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Dilution
Overall, 84% of participants reported that they have further diluted certain adult IV push medications prior to administration. These findings are similar to our 2014 survey in which 83% of respondents further diluted certain IV push medications. However, the frequency of dilution has decreased since 2014 (Table 2). Pertaining to the containers in which IV medications are provided, medications available in single-dose vials were most often diluted in both the 2014 and 2018 surveys. Yet, as many as 1 in every 5 participants still reported in 2018 that they sometimes, often, or always dilute medications provided in multiple-dose vials (21%) or manufacturer’s prefilled syringes (16%). Dilution was least frequent with pharmacy-dispensed syringes that contain patient-specific doses (6%). While the frequency of dilution has decreased, the practice continues.
| Container Type | Percent of Respondents | Most Frequent Medications Diluted (2018 Survey Only) | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Year | Never 0% | Rarely 1-10% | Sometimes 11-50% | Often 51-95% | Always >95% | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Manufacturer’s prefilled syringe | 2014 | 42 | 15 | 18 | 15 | 10 | Opioids, anxiolytics/anti-psychotics, antiemetics, diphenhydrAMINE, cardiovascular agents, ketorolac | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2018 | 70 | 14 | 11 | 4 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pharmacy syringe with patient- specific dose | 2014 | 63 | 17 | 8 | 7 | 5 | Opioids, anxiolytics/anti-psychotics, antiemetics, cardiovascular agents, antibiotics, cortico-steroids | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2018 | 86 | 8 | 4 | 1 | 1 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Single-dose vial | 2014 | 9 | 14 | 35 | 28 | 14 | Opioids, antiemetics, anxiolytics/antipsychotics, antibiotics, diphenhydr-AMINE, ketorolac | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2018 | 16 | 25 | 37 | 18 | 4 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Multiple-dose vial | 2014 | 36 | 15 | 23 | 15 | 11 | Opioids, antiemetics, anxiolytics/antipsychotics, cardiovascular agents, diphenhydrAMINE, antibiotics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2018 | 65 | 14 | 14 | 5 | 2 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In our 2018 survey, opioids, anxiolytics/antipsychotics, and antiemetics were the most frequently diluted medications, regardless of the container in which the medication was provided. In fact, approximately three-quarters of participants reported further dilution of opioids provided in both commercially available (78%) and pharmacy-dispensed (69%) prefilled syringes. Anticonvulsants, naloxone, insulin, and heparin were the least frequently diluted medications in the survey. Medications that were not included in the survey but frequently mentioned as being diluted included famotidine and pantoprazole.
Among participants who dilute adult IV push medications prior to administration, 81% confirmed that they have used a prefilled 0.9% sodium chloride (saline) flush syringe (commercially or pharmacy-prepared) for this purpose. Approximately 56% said they use a flush syringe to dilute medications at least half of the time, and 19% said they always do. When describing this practice, most participants did not include relabeling of the flush syringe. This unsafe practice has increased in frequency since our 2014 survey, at which time 54% of practitioners said they had diluted medications using a saline flush syringe. One possible reason for the increase may be the shortage of vials of 0.9% sodium chloride at the time of the survey, which many practitioners noted in the comments section.
The primary factors that influenced a decision to further dilute adult IV push medications were associated with the desire to administer the drug slowly (94%), avoid patient discomfort (70%), reduce the risk of extravasation (33%), and measure small volume doses accurately (25%). Other reasons (13%) included drug-specific requirements (e.g., LORazepam), facility policies, recommendations in drug references, and prior education.
Labeling
Only half (50%) of the participants told us they always label IV push medications that are self-prepared away from the patient’s bedside. Comments suggest that labeling was sometimes accomplished by taping the vial to the syringe. More than a quarter (28%) of participants said they rarely or never label these syringes. Participants who said they did not always label syringes prepared away from the patient’s bedside told us that labeling was not necessary if they prepared just one medication (51%) or one syringe (45%) (Table 3). Surprisingly, 7% of participants said they could even distinguish between multiple syringes without a label by visual appearance or location of the syringe. Among these participants, the most frequent ways of distinguishing between two or more unlabeled syringes was by the different volumes of medication in each syringe (76%); the size of the syringes (40%); differences in needles, caps, or medication colors (36%); orientation on a tray or sterile field (16%); or by carrying syringes in different hands (12%) or pockets (12%).
| Reason | Percent of Respondents | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not necessary if I prepare only one medication | 51 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not necessary if I prepare only one syringe | 45 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Emergency | 39 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Too time consuming | 20 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| No labels available | 20 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not an expectation | 12 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Not necessary because I can distinguish syringes by visual appearance or location | 7 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Impact of Drug Shortages
Given the continuing drug shortage crisis, approximately one-third of participants agreed or strongly agreed with these statements:
- I am giving more medications via IV push that were previously given as infusions, particularly antibiotics, antiemetics, and proton pump inhibitors (38%)
- I am required to prepare more IV push medications at the bedside, or wait longer for pharmacy preparation and dispensing (34%)
- IV push drugs are being provided in unfamiliar formulations (concentrations and packages), or in volumes greater than needed for each dose (31%)
- I get less prefilled, ready-to-administer syringes than previously, particularly in the correct concentrations or volumes (31%)
Comments suggest that drug shortages also result in adverse outcomes such as delays in therapy due to pharmacy preparation of products in short supply, and drug waste. Even when medications are provided in prefilled syringes, the amount of drug in the syringe is often more than the patient’s dose, leading to product waste along with using additional staff time to document the wasting of drugs such as opioids. Numerous participants said it seemed like they waste more medications than ever during drug shortages.
Learning to Administer and Dilute IV Push Medications
Most participants learned how to administer IV push medications during their professional training (79%), during orientation with their first professional position (56%) and/or current position (32%), from drug references (43%), and from on-the-job experiences (35%).
Approximately half of participants were taught to dilute adult IV push medications during their professional training (53%) or during orientation to their first professional position (47%). About a quarter of participants were taught this practice during orientation to their current position (29%), and more than one-third learned it from on-the-job experiences (39%) or drug references (38%). Only 9% reported receiving no formal instructions on diluting adult IV push medications.
Determining and Controlling the Rate of Administration
Only about two-thirds (63%) of participants indicated that the rate of administration of an IV push medication is provided on the patient’s medication administration record or electronic health record. Many participants said they need to look up the rate of administration in drug references (41%), in facility-specific guidelines (40%), or remember the rate from previous administrations (41%). Eighteen percent of participants reported that they administer all IV push medications over 2 to 5 minutes, so they don’t need to look up or know the specific rate of administration for each drug. A few reported they administer all IV push medications in less than 2 minutes. To control how fast they are administering IV push medications, 82% use a clock, watch, phone, or other timing device. To administer the dose over the desired timeframe, 38% stated that they give small incremental doses frequently, whereas 30% said they just apply constant pressure on the plunger.
Conclusions
Most participants in the recent survey do not receive IV push medications in ready-to-administer syringes and must prepare these medications prior to administration, which has only become more common during the ongoing drug shortage crisis. Various unsafe practices associated with preparing and administering IV push medications have been reported in our 2018 survey, including the withdrawal of medications from one syringe (or cartridge) and transferring to another syringe, a practice that has increased in frequency compared to our 2012 survey. Dilution is the most common reason for withdrawing a medication from the prefilled syringe. Although the frequency of diluting IV push medications has decreased since 2014, the practice continues.
When dilution occurs, most practitioners have used a saline flush syringe for this purpose, an unsafe practice that has also increased since our 2014 survey. Although further dilution is often not necessary, the decision to dilute is often guided by a desire to administer the dose slowly to avoid adverse effects, reduce patient discomfort at the administration site, prevent extravasation, and measure small doses accurately. Unfortunately, saline flush syringes that contain a medication are rarely relabeled. Finally, more than a quarter of survey participants reported that they rarely or never label IV push medications that have been prepared away from the bedside.
While these unsafe practices associated with IV push medication administration have been widespread for years, the drug shortage crisis has likely contributed to their ongoing occurrence. Also, from our survey it seems that some of these unsafe practices are taught during training, orientation, or on-the-job experiences, perpetuating their occurrence.
In Part II, we will provide recommendations to improve the safety of adult IV push medication administration, based on the vulnerabilities identified in the 2018 survey.
References
- ISMP. ISMP survey on IV push medication practices. ISMP Medication Safety Alert! Nurse AdviseERR. 2018;16(7):4-5.
- ISMP. Survey shows recession has weakened patient safety net. ISMP Medication Safety Alert! 2010;15(1):1-4.
- ISMP. ISMP survey reveals user issues with Carpuject prefilled syringes. ISMP Medication Safety Alert! 2012;17(16):1-3.
- ISMP. Some IV medications are diluted unnecessarily in patient care areas, creating undue risk. ISMP Medication Safety Alert! 2014;19(12):1-5.
- ISMP. ISMP safe practice guidelines for adult IV push medications. 2015.
- INS (Infusion Nurses Society). Infusion therapy standards of practice (standard 40, flushing and locking, practice criteria D3). J Infus Nurs. 2016;39(1S):S1-S159.