
Promethazine Conundrum: IV Can Hurt More Than IM Injection!
In our August 10, 2006 newsletter, we highlighted the well-known,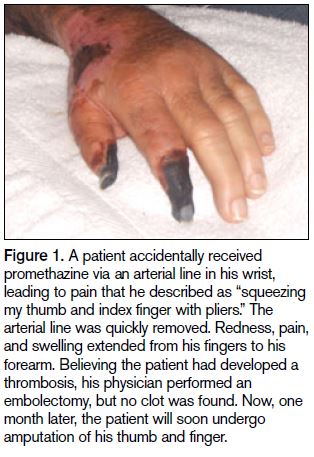 caustic effects of promethazine and suggested ways to reduce the risk of serious tissue injuries and amputations from inadvertent arterial injection or IV extravasation. This topic evoked considerable response from the media and readers who contacted us with comments about our recommendations along with troubling stories of their own about serious injuries from promethazine extravasations (see Figure 1).
caustic effects of promethazine and suggested ways to reduce the risk of serious tissue injuries and amputations from inadvertent arterial injection or IV extravasation. This topic evoked considerable response from the media and readers who contacted us with comments about our recommendations along with troubling stories of their own about serious injuries from promethazine extravasations (see Figure 1).
In response to this heightened attention, we invited readers to participate in a survey published in our August 24, 2006, newsletter to learn more about the scope of the problem and to prioritize our injury prevention strategies. From the nearly 1,000 survey responses and many additional unsolicited comments we received, two things were abundantly clear:
- Promethazine extravasations that result in serious tissue damage are not rare; indeed, one in five respondents reported awareness of such an occurrence in their facility within the past 5 years
- While healthcare providers are frustrated with this longstanding problem for which there is no easy solution, many have been inspired to revisit the issue and take new measures to reduce the risk of patient injury from IV promethazine.1
Survey findings. Among the recommendations we suggested in our survey to reduce the risk of tissue injuries, most were deemed to be of great value by respondents, particularly: diluting the drug; limiting the concentration and initial dose; providing alerts on medication administration records (MARs) and automated dispensing cabinet (ADC) screens; injecting the drug into a running IV using the port furthest from the patient’s vein; and advising patients to report any IV site discomfort. Yet, implementation of these recommendations was much lower than expected, considering their perceived value (see Table 1).
| Recommendation | Value (1=low, 5=high) | % Follow recommendation |
|---|---|---|
| Dilute the drug in 10 to 20 mL of saline | 4.5 | 47 |
| Advise patients to report burning/pain | 4.5 | 59 |
| Limit concentration to 25 mg/mL | 4.3 | 69 |
| Alerts about safety precautions on MARs | 4.3 | 27 |
| Alerts about safety precautions on ADC screens | 4.2 | 19 |
| Inject drug through running IV line | 4.1 | 41 |
| Safety requirements in standing orders | 4.1 | 22 |
| Inject in port furthest from patient's vein | 4 | 24 |
| Limit starting dose to 6.25 - 12.5 mg | 4 | 29 |
| Administer slowly over 10 minutes | 3.8 | 26 |
| Remain with patient to assess IV site | 3.8 | 33 |
| Do not administer via hand/wrist veins | 3.7 | 10 |
| Use alternative rescue antiemetics | 3.5 | 38 |
| Prepare drug in saline minibags | 3.3 | 10 |
| Give drug through central venous site only | 2.8 | 4 |
| Ban IV use of promethazine | 2.4 | 3 |
| Remove promethazine from the formulary | 2.3 | 3 |
While about two-thirds of all respondents limit promethazine concentration to 25 mg/mL, only about half of all respondents dilute the drug in 10 to 20 mL of saline, inject it through a running line, and advise patients to report IV site discomfort. Only about a quarter limit the starting dose to 6.25 to 12.5 mg, provide alerts on MARs, and use the furthest port when injecting the drug. Just one-fifth of all respondents provide alerts on ADC screens. Even more surprising, just one-third of all respondents expect staff to remain with the patient during administration to assess the IV site, and only one-quarter require slow administration over 10 minutes, although two-thirds clearly felt these actions were valuable (respondents chose 4 or 5, with 5 being the highest value). About half of all respondents agreed that IV promethazine should never be administered via hand or wrist veins, but just 10% reported following such a policy. Recommendations that would eliminate the use IV promethazine and remove it from the formulary received the lowest scores for both perceived value and current implementation, perhaps because there are so few alternatives as effective as IV promethazine. Nonetheless, Table 2 provides a list of drugs from the 38% of respondents who reported using alternative antiemetics instead of IV promethazine.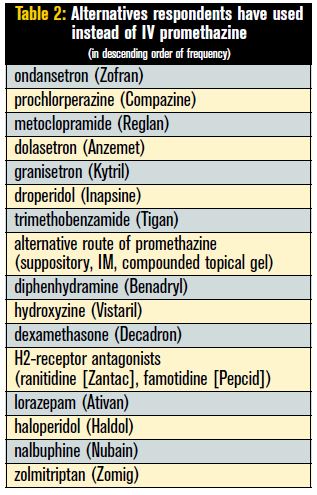
This survey and responses to our initial article brought to light some concerns about our recommendations, as well as new ideas for managing the risk of tissue injury.
Concerns. Several practitioners expressed concern about our reference to promethazine as a “known vesicant” in our August 10, 2006 article. While other credible sources have also suggested that the drug is a “vesicant,” the package insert for PHENERGAN and promethazine refers to the drug as an “irritant.”2,3 Thus, we agree that “vesicant” may have been used injudiciously to describe promethazine. However, some hospitals have added promethazine to their list of “vesicants,” primarily to promote awareness and facilitate proper risk reduction efforts.
Several practitioners were also concerned that preparing promethazine in a saline bag and administering it over 10 minutes or more would require the use of an infusion pump, potentially leading staff to believe they do not need to remain at the bedside to observe the IV site. Thus, current policies on the use of infusion pumps and conditions that require constant monitoring may need revisions to promote safe administration of IV promethazine. While the rate of infusion may not be directly associated with the tissue damage that results from extravasation, a dilute drug administered very slowly allows for quick discontinuation of the injection if the patient complains of pain. Very slow administration also reduces the risk of extravasation in small, fragile veins.
Another pharmacist questioned the use of ondansetron and other 5-HT3 agents as an alternative for IV promethazine as a rescue antiemetic. These drugs are typically used to prevent nausea and vomiting during chemotherapy or radiation therapy. During such treatments, serotonin (5-HT) is released from the gastrointestinal tract, which stimulates vagal neurons to transmit a signal to the vomiting center in the brain. 5-HT3 agents bind to the vagal neuron receptors, thus blocking the signal to vomit. As such, these drugs are most effective if they are administered before treatment, or before the patient becomes nauseated, and thus may not be effective as a rescue antiemetic. The pharmacist also pointed out that higher doses of 5-HT3 agents can increase the QT interval and cause cardiac arrhythmias.
One practitioner questioned whether serious tissue injury occurs primarily with inadvertent arterial injections rather than IV extravasations. However, we have anecdotal evidence, many reports from the USP-ISMP Medication Errors Reporting Program, and cases in the literature4 that also confirm serious injury from IV extravasation.
Additional recommendations. Some facilities reported additional strategies not mentioned in our survey or article. One pharmacist reported that he now dispenses each vial of promethazine in a small ziplock bag with an insert that contains instructions for safe administration along with a photo of actual tissue damage, taken from our August newsletter. Although the pharmacy also prints alert messages on MARs, these warnings are not available to staff in the ED or OR, so the attention-grabbing photo and information in the bag are the primary means of communicating precautions.
Another hospital reported that, in addition to prohibiting administration of promethazine through IV sites in the hand and wrist, nurses no longer give the drug through an IV in the antecubital space, where nerves, arteries, and veins are very close. Whenever possible, they use an IV site on the back of the arm unless the patient has a central line.
Several hospitals have told us about nausea and vomiting prevention protocols they use to reduce the use of IV promethazine. For example, one pharmacist reported that patients receive ranitidine and dexamethasone preoperatively, and dolasetron 30 minutes before the end of surgery. Promethazine IV is used only as a last resort.
Conclusion. Only 24% of respondents believe FDA should withdraw approval for the IV route of administration of promethazine. As such, healthcare providers need to review their current practices associated with the administration of IV promethazine and establish safeguards to prevent inadvertent arterial injection and IV extravasation. An ED physician aptly affirmed both the desire to preserve IV use of promethazine and the need to address its risks in the following message to ISMP:
For 27 years, I have used IV promethazine 2 to 3 times every shift I work. I have personally never seen serious tissue damage or other major problems with this medication, aside from rare instances of local phlebitis that have resolved without incident. This is not to underestimate the serious risks of using this medication, mostly associated with inadvertent intra-arterial injection or tissue infiltration, but to underscore the fact that all medications have risks/benefits. In my opinion, the benefits far outweigh the risks with IV promethazine…I have seen many good drugs go out of favor because of reported problems, which have almost always been disproportionate to their benefits. Most of these have been related to improper use or administration. Let’s face it: life decisions in general, and the practice of medicine in particular, always involves risks and benefits. Let’s not ignore the risks, but let us also keep the benefits in perspective!
Thanks to all who completed the survey and those who sent messages to us about this complex issue. We hope that our recent article and survey have brought sufficient attention to this longstanding problem to drive needed changes in practice around the administration of IV promethazine.
References:
- Friederich S. Westport woman settles hospital suit. The Daily World. August 30, 2006:
- Phenergan (promethazine HCl) injection package insert. Deerfield, IL: Baxter Healthcare Corporation; 2005
- Promethazine hydrochloride injection [package insert]. Irvine, CA: Sicor Pharmaceuticals Corp; 2004.
- Malesker MA, Malone PM, Cingle CM, Cochran RM. Extravasation of IV promethazine. Am J Health-Syst Pharm 1999; 56: 1742-43.