
Should FDA Reconsider Allowing the Pooling of COVID-19 Vaccine Doses to Obtain Additional Doses?
ISMP thanks Kevin N. Hansen, PharmD, MS, BCPS, BCSCP, from the Moses H. Cone Memorial Hospital in Greensboro, North Carolina, for contributing this article.
ISMP joins the author and others who encourage FDA to reconsider the safe and responsible pooling of COVID-19 vaccines...
Vaccinators have observed remaining residual volume in the current coronavirus disease 2019 (COVID-19) vaccine vials (Figure 1) after obtaining the full labeled quantity of doses available from each vial (Table 1) and have expressed a desire to pool the leftover vaccine to obtain an additional full dose for administration. This practice would have the potential to increase the number of Americans who could be vaccinated with the existing supply and prevent unnecessary vaccine wastage. The US Food and Drug Administration (FDA) has advised that “…any further product remaining that does not constitute a full dose should not be pooled from multiple vials to create one.”1 This has created frustration as vaccinators continue to witness potential additional vaccine doses go to waste coupled with the existing challenges of limited vaccine supplies. This presents an opportunity to review the practice of drug pooling, drug preservatives, contamination risks, aseptic technique, and future directions to maximize the doses withdrawn from vaccine vials.

Table 1. Current FDA Emergency Use Authorization (EUA) COVID-19 Vaccines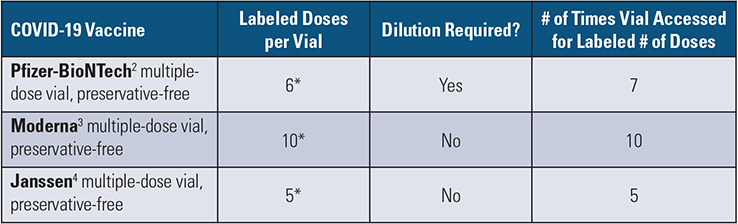
* Reports have demonstrated that additional full doses may be present if using certain low dead-volume (LDV) syringes and needles; withdrawing these additional doses would require additional vial access.
Drug Pooling Defined
Drug pooling is the act of combining the volume from multiple drug vials into a container or syringe to obtain a specified dose for administration. This is a routine practice for many drugs, both with and without preservatives, prepared in ISO (International Organization for Standardization) classified pharmacy cleanrooms within a primary engineering control, such as a laminar airflow workbench, that provides ISO class 5 unidirectional airflow in a controlled environment. These engineering controls are critical to prevent the contamination of the sterile drug when proper aseptic technique is used and to reduce the risk of potential harm to the patient.
Multiple-Dose Vials and Preservatives
The current FDA Emergency Use Authorization (EUA) COVID-19 vaccines (i.e., Pfizer-BioNTech, Moderna, Johnson & Johnson’s Janssen) are each labeled as multiple-dose vials. Drugs labeled as multiple-dose vials usually contain a preservative at high enough concentrations to kill or slow the growth of microbial contamination during the drug extraction process,5 allowing extended use time after the vial stopper has been penetrated and numerous withdraws of vial contents using a needle and syringe. However, while the COVID-19 vaccines are labeled as multiple-dose vials, they do NOT contain any preservatives. For this reason, the current EUA for each vaccine explicitly states, “Do not pool excess vaccine from multiple vials”2-4 due to the contamination risks from accessing a vial multiple times.
Excess Volume and Drug in COVID-19 Vials
For injectable medications in solution, manufacturers provide minimal amounts of excess volume and drug in each vial (Table 2). These excess volumes are usually sufficient to permit withdrawal and administration of the labeled amounts and volumes.6 With the overfill, the COVID-19 vaccines may have excess vaccine and volume remaining in the vial after the labeled number of doses have been removed.
Table 2. Recommended Excess Volumes (Overfill) for Injectable Medications
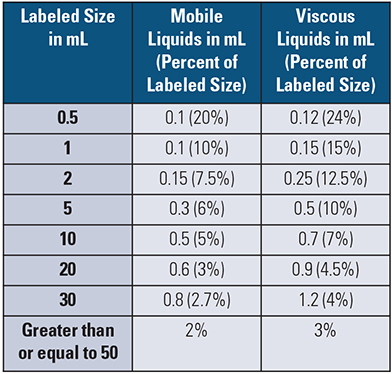
Source: USP General Chapter <1151> Pharmaceutical Dosage Forms6
Low Dead-Volume Syringes and Needles
When preparing and administering the COVID-19 vaccines, there are a myriad of syringe and needle combinations that can be used, each with varying levels of dead space. The use of low dead-volume (LDV) syringes for vaccine preparation during a pandemic is not novel; however, the impact of their use should not be underestimated, as visually displayed in Table 3 using the Pfizer-BioNTech COVID-19 vaccine as an example. Furthermore, since the COVID-19 vaccinations require intramuscular (IM) injections, the needle length and gauge may vary based on the patient’s age, gender, and weight, as recommended by the Centers for Disease Control and Prevention (CDC). This can affect the amount of liquid remaining in the needle after vaccine administration.7
Table 3. Impact of Using Low Dead-Volume (LDV) Syringes for the Pfizer-BioNTech COVID-19 Vaccine2
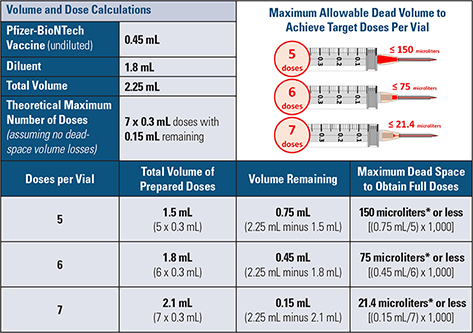
*1 microliter equals 0.001 mL
In 2006, Strauss et al. described “the critical role of the syringe” during a pandemic, such as an influenza pandemic, and found that an LDV syringe could provide up to 19% additional vaccine (influenza) doses per vial when 10-dose vials were used.8 This could equate to thousands or even millions of additional people becoming vaccinated during mass campaigns and ultimately reduce morbidity and mortality during a pandemic. The authors state explicitly, “It is therefore of paramount importance to stock a syringe which will reduce vaccine wastage to a minimum and thereby allow the greatest number of persons to be vaccinated.”8
Potential Risks with Pooling COVID-19 Vaccines
There are several potential risks with pooling the current COVID-19 vaccines that must be considered, including the first two previously discussed:
-
Lack of Controlled Environment: A cleanroom or hood with an ISO class 5 environment is currently not required for dilution or preparation of COVID-19 vaccine doses.9 Non-controlled environments are expected to be contaminated with bacteria and fungus in the air and on surfaces. Aseptic technique can minimize contamination but cannot eliminate the risk of contamination.
-
Lack of Preservatives: The vaccines are labeled as multiple-dose vials but do NOT contain any preservatives. Each access into the vial is an opportunity to contaminate the vaccine. Contaminated drug products have a higher propensity to cause patient harm.10
-
Vial Coring: With each vaccine, the vial’s rubber stopper is accessed multiple times with a needle. The integrity of the vial stopper diminishes after each needle puncture, increasing the risk of introducing pieces of the rubber stopper or other particulates into the vaccine.
-
Suspension: Each of the current COVID-19 vaccines are suspensions requiring careful vial inversion prior to withdrawing a dose to uniformly distribute the active ingredient. There is a theoretical risk of combining vaccines from multiple vials that could have slightly varying levels of uniformity. Combining the vials may amplify this effect, creating a possible subpotent or superpotent dose.
-
Mixing Lots: Pooling vaccine doses across multiple vials may result in inadvertently mixing vaccines with different lot numbers. This has implications for proper documentation of vaccine administration to the patient, poses challenges with recalls or adverse event reporting, and may impact how vaccine supply is communicated to individual states, impacting potential future vaccine supply allocation.
-
Beyond-Use Date: The allowable beyond-use date (BUD) for diluted/punctured COVID-19 vaccine vials or pre-drawn syringes is 6 hours at room temperature (Pfizer-BioNTech, Moderna) and 6 hours refrigerated (Janssen). These BUDs are generous when compared to the 1 hour BUD currently allowed using the “immediate-use” provision when prepared outside of controlled environments in the USP General Chapter <797> Pharmaceutical Compounding-Sterile Preparations.11 Furthermore, even when compounded sterile preparations (CSPs) are prepared within a controlled environment, the risk is elevated from ‘low-risk’ to ‘medium-risk’ when using more than two entries into any one sterile container. The COVID-19 vaccines are accessed a minimum of five times and as many as 10 times per single vial.
Should the FDA Allow Pooling?
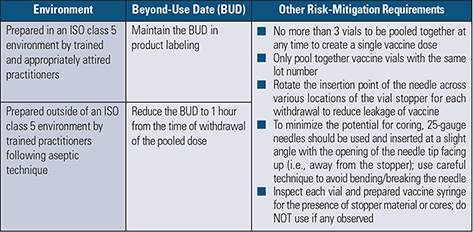
Because the stated concerns associated with contamination and lack of preservatives can be mitigated by preparing the vaccine doses in an ISO class 5 environment and/or reducing and limiting the BUD, we believe FDA should further evaluate and reconsider whether the pooling of the current COVID-19 vaccines can be accomplished in a safe and responsible manner through risk-mitigation strategies of the process, such as those suggested in Table 4.
Table 4. Examples of Risk-Mitigation Strategies for FDA Consideration to Allow Safe Pooling of COVID-19 Vaccines
ISMP joins the author and many other practitioners who encourage FDA to evaluate and reconsider the safe and responsible pooling of COVID-19 vaccines, as suggested above. If pooling is approved, FDA, with USP, should provide specific details and guidance on a safe approach to pooling each of the current COVID-19 vaccines. For example, presented below are two different approaches to pooling the Pfizer-BioNTech vaccine, with the limitations noted for each approach.
Serial Approach: After dilution, the vaccinator withdraws 6 full doses from each vial. But upon withdrawal of dose 7, only 0.1 mL can be drawn into the syringe (need 0.3 mL for each full dose). The vaccinator then uses another full vial from the same lot and completes the dose, taking 0.2 mL out of the vial. The vaccinator continues to prepare syringes using that vial; however, they can now get only 5 full doses from the vial, with 0.2 mL remaining. The vaccinator withdraws the 0.2 mL into a syringe, and completes the dose using another full vial from the same lot, and so on.
-
Limitations: This approach may be risky; if the vaccine in the vial is contaminated during the process, essentially every dose withdrawn from the vial and future vials would be contaminated.
Residual Volume Approach: After dilution, the vaccinator withdraws 6 full doses from each of 3 vials (18 full doses). Each used vial contains about 0.1 mL of residual, withdrawable volume. The vaccinator then withdraws the residual volume from the 3 vials until a full dose is achieved.
-
Limitations: This method would not lead to a serial contamination issue; however, using a single needle to access 3 vials can cause blunting of the needle (which can result in pain when using the same needle for administration), as well as increase the risk of coring the rubber stopper. Also, the residual volume present in the vial is highly variable and dependent on the specific syringes and needles used during the preparation.
An additional limitation for pooling using either approach—coupled with the option to prepare doses outside of an ISO class 5 environment—is that it will be challenging to ensure the pooled doses receive the appropriate BUD. A well-designed process for differentiating and separating the syringes that have different BUDs will be important for vaccinators to consider.
Considerations for Syringe and Needle Manufacturers
Syringe and needle manufacturers should consider mass producing LDV syringes (dead space less than or equal to 21.4 microliters) with affixed needles. They should ensure that they are easy to use, contain a needle safety mechanism, have affixed 25-gauge needles, offer varying needle lengths based on the CDC’s recommendations for IM injections, and are produced in sufficient quantities to expedite the end of this pandemic.
Next Steps and Recommendations
ISMP, the author, and many other practitioners suggest reconsideration of pooling vaccine doses with good intent—to vaccinate more of the public to end this pandemic. However, we should not sacrifice quality and/or the safety of our patients in this process. In the interim, practitioners should maximize the number of doses withdrawn from each vaccine vial with the use of LDV syringes and needles, prepare vaccines using proper aseptic technique, and continue to get vaccinations into patients’ arms.
References
- US Food and Drug Administration (FDA). Pfizer-BioNTech COVID-19 vaccine frequently asked questions. January 28, 2021.
- Pfizer-BioNTech COVID-19 Vaccine. Fact sheet for healthcare providers administering vaccine (vaccination providers). Emergency use authorization (EUA) of the Pfizer-BioNTech COVID-19 vaccine to prevent coronavirus disease 2019 (COVID-19). New York, NY: Pfizer; 2021.
- Moderna COVID-19 Vaccine. Fact sheet for healthcare providers administering vaccine (vaccination providers). Emergency use authorization (EUA) of the Moderna COVID-19 vaccine to prevent coronavirus disease 2019 (COVID-19). Cambridge, MA: Moderna; 2020.
- Janssen COVID-19 Vaccine. Fact sheet for healthcare providers administering vaccine (vaccination providers). Emergency use authorization (EUA) of the Janssen COVID-19 vaccine to prevent coronavirus disease 2019 (COVID-19). Horsham, PA: Janssen; 2021.
- Meyer BK, Ni A, Hu B, Shi L. Antimicrobial preservative use in parenteral products: past and present. J Pharm Sci. 2007;96(12):3155-67.
- United States Pharmacopeia and the National Formulary (USP 43-NF 38). USP General Chapter <1151> Pharmaceutical Dosage Forms. Rockville, MD; August 2020. Accessed: March 16, 2021.
- Centers for Disease Control and Prevention (CDC). Vaccine administration: needle gauge and length. August 4, 2020.
- Strauss K, van Zundert A, Frid A, Costigliola V. Pandemic influenza preparedness: the critical role of the syringe. Vaccine. 2006;24(22):4874-82.
- USP. COVID-19 vaccine handling toolkit: operational considerations for healthcare practitioners. March 2021. Version 3.0.
- US Department of Health and Human Services, FDA, Center for Drug Evaluation and Research Office of Compliance. Insanitary conditions at compounding facilities: guidance for industry. November 2020.
- USP-NF (USP 43-NF 38). USP General Chapter <797> Pharmaceutical Compounding—Sterile Preparations. Rockville, MD; May 2020. Accessed: March 16, 2021.
Access this Free Resource
You must be logged in to view and download this document.