
Subtherapeutic Heparin Infusions: Is Your Organization at Risk of Bypassing Soft Low-Dose Alerts?
Problem: We recently received a report from a large health system about a trend related to misprogramming continuous intravenous (IV) heparin infusions administered via smart infusion pumps. The misprogramming resulted in significant subtherapeutic doses of heparin for multiple patients, increasing their risk of serious thromboembolic complications. In this health system, more than 90% of all continuous IV heparin infusion doses are weight-based, using standardized, indication-based heparin protocols to determine the patient’s initial bolus dose and infusion rate, as well as any required dose changes based on regular blood coagulation measurements (e.g., aPTT, anti-Factor Xa). A typical heparin starting dose might include a bolus dose of 60 to 80 units per kg followed by an infusion rate of 12 to 18 units per kg per hour, depending on the indication.
Interoperability not implemented in the ED and surgical/procedural areas
About a year ago, this health system had implemented interoperability between its electronic health record (EHR) (Epic) and smart infusion pumps (BD Alaris). However, the misprogrammed heparin infusion events had occurred in the two patient care areas where interoperability had not been initiated—the emergency department (ED) and surgical/procedural areas. Interoperability had not been implemented in surgical/procedural areas due to technical incompatibilities between the EHR order workflow and the pump interoperability platform. The necessary workflow for practitioners to use barcode scanning to associate the smart pump with a medication infusion order, and then to send the order parameters to the pump, had not been developed. In the ED, interoperability had not been established initially due to limitations in the EHR, which have since been corrected. More recently, the primary barrier to interoperability in the ED is an inadequate supply of smart infusion pumps and channels for administration of all IV plain solutions and non-critical medications via a smart pump.
Smart infusion pump-EHR interoperability enables the infusion parameters ordered by the prescriber, which have been reviewed by a pharmacist, to pre-populate the smart infusion pump screen, thereby reducing the risk of manual programming errors.1 The pump settings must then be confirmed by a nurse or other user prior to starting the infusion. Interoperability also facilitates the automatic documentation of infusion data in the EHR. According to analysis of infusion pump errors submitted to the ECRI Patient Safety Organization (PSO), up to three-quarters of the pump programming errors associated with primary infusions could have been averted with successful pump interoperability, as long as the associated pump warnings were heeded.2
Misprogrammed heparin infusions
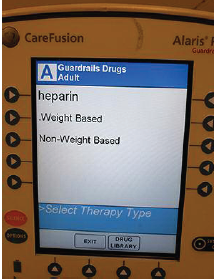
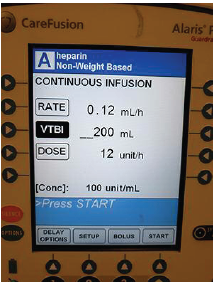
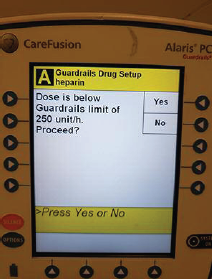
A pharmacist from one hospital in the health system had received a report of an error with a heparin infusion that had occurred in the ED, where nurses needed to manually program smart infusion pumps. During the event investigation, it was found that once “heparin” was selected within the drug library, the nurse was presented with a screen for selecting whether the heparin infusion would be “weight based” or “non-weight based” (Figure 1). The misprogramming error began at this initial step, with selecting a “non-weight based” heparin infusion instead of a “weight based” heparin infusion. This resulted in a significant subtherapeutic dose: the pump was programmed to deliver only 12 units per hour (Figure 2) for an 80 kg patient who was supposed to receive heparin 12 units per kg per hour (960 units per hour). Because the dose error-reduction system (DERS) was engaged, the smart infusion pump issued a soft low-dose alert (Figure 3), which was overridden by the nurse. Unlike maximum dose alerts and low concentration alerts, low-dose alerts cannot be configured as hard stops within the BD Alaris (CareFusion) pumps. Thus, the heparin infused at a low rate of 12 units per hour (0.12 mL per hour).
Trend identified
The pharmacist investigating this error remembered a similar programming error with heparin that had happened recently. She asked rotating student pharmacists to help conduct a small study to identify similar errors that may be happening systemwide. The students ran a basic systemwide smart infusion pump data report to identify all adult heparin infusions that were initially infused at a rate less than 1 mL per hour (100 units per hour), since these low-rate infusions all represented errors. The data report identified more than 70 low-rate infusions within a 2-month period. Further analysis showed that users had initially selected “non-weight based” heparin in error and entered a low dose per hour. They then overrode the soft warning about the low dose. Within a minute, however, two-thirds of the users realized their error and reprogrammed the pump to correctly deliver the prescribed heparin dose.
The pharmacist and students then reviewed all cases in which the subtherapeutic heparin dose (less than 1 mL [100 units] per hour) continued for at least 20 minutes. In a 2-month period, they identified 25 cases in 3 hospitals in which the heparin infusion ran for at least 20 minutes as units per hour instead of units per kg per hour. The longest subtherapeutic heparin infusion continued for more than 28 hours. Because the pump data were not linked to specific patients, the pharmacist and students were unable to determine if the patients who received these subtherapeutic doses were harmed. However, heparin is a high-alert medication, and both under- and overdoses can lead to significant patient harm.
Safe Practice Recommendations: To reduce the risk of heparin infusion errors related to the misprogramming of a smart infusion pump, consider the following recommendations:
Review smart pump data. If you permit both weight-based and non-weight-based dosing of heparin infusions within the same drug library, analyze your smart infusion pump data to determine if similar programming errors have occurred in your facility. Organizations that employ smart infusion pumps should provide dedicated time and resources for regular review and analysis of pump data (at least quarterly) to assess how medications (e.g., heparin) and solutions are being administered, and to improve overall medication safety.1,3
Heparin weight-based dosing. Standardize to only weight-based dosing for heparin infusions. Eliminating non-weight-based dosing of heparin will reduce the risk of inadvertently administering infusions as units per hour instead of units per kg per hour. If there are specific indications for which standard weight-based heparin dosing is not feasible, limit the non-weight-based heparin infusion programming choice to the appropriate care area/profile where it is needed.
Configure heparin low-dose hard stops (when possible). Establish a hard stop for low-dose alerts with heparin if your smart infusion pump allows such configuration. The health system that noted a trend with subtherapeutic heparin infusion dosing has shared its smart infusion pump study data with BD Alaris and asked the company to allow a hard stop for minimum doses of certain high-alert medications, including heparin. ISMP has also been in contact with BD to request this capability. In the meantime, educate nurses about the potential significance of low-dose alerts and to consider the consequences of subtherapeutic heparin doses. Low-dose alerts may signal a programming error and should trigger a full review (and independent double check—see below) of the pump programming before proceeding. At least quarterly, all overridden smart pump alerts (high- and low-dose limits) should be reviewed for appropriateness.1
Implement interoperability. Implement bi-directional (i.e., auto-programming and auto-documentation) smart infusion pump interoperability with the EHR. See the ISMP Guidelines for Optimizing Safe Implementation and Use of Smart Infusion Pumps1 for comprehensive recommendations associated with adopting interoperability. Also ensure that an adequate supply of smart infusion pumps (and channels) is available for use in all clinical areas, including in the ED and surgical/procedural areas. Organizations that have implemented interoperability in the ED have excluded “out of scope” medications/infusions that are emergent in nature, such as those used during code blues, rapid responses, or trauma care, and timely thrombolytics for stroke patients. After managing these emergencies, the infusion is then linked to the EHR. Use of interoperability in the surgical and procedural areas is supported by some EHRs and pump interoperability platforms but may not be feasible in your facility at this time depending on restrictions with existing workflow, space, and technology platforms. However, please see our March 12, 2020, newsletter3 regarding implementation of smart infusion pumps with an engaged drug library in the operating room as a first step towards interoperability in the surgical setting.
Independent double check for user-programmed heparin infusions. If user-programming of infusion pumps is necessary, consider requiring an independent double check of all programming parameters (as well as verification of the patient, patient’s weight, drug [concentration and dose rate], line attachment, and lab values upon which dosing is based) before administering heparin infusions. For hospitals that may not have a second nurse readily available to perform an independent double check, a pharmacist could be called instead to confirm all calculations and dosing, and to verbally review all concentration, dose, and rate settings, as they appear on the pump screen, with the nurse.
References
- ISMP. Guidelines for optimizing safe implementation and use of smart infusion pumps. 2020.
- ECRI. Guidance article. Infusion pump integration. Health Devices. 2013;42(7):210–21.
- ISMP. Do you know what doses are being programmed in the OR? Make it an expectation to use smart infusion pumps with DERS. ISMP Medication Safety Alert! 2020;25(5):1-5.
Access this Free Resource
You must be logged in to view and download this document.