
Survey Shows Room for Improvement with Two New ISMP Targeted Medication Safety Best Practices
In our February 27, 2020 newsletter, we invited hospitals to participate in a short survey to establish a baseline level of implementation for two new Best Practices released in the 2020-2021 ISMP Targeted Medication Safety Best Practices for Hospitals. The purpose of the Targeted Medication Safety Best Practices is to identify, inspire, and mobilize widespread, national adoption of consensus-based Best Practices to address recurring problems that continue to cause harmful and even fatal errors despite repeated warnings in ISMP publications. The two new Best Practices for 2020-2021 are associated with safely prescribing extended-release (ER) and long-acting (LA) opioids and minimizing the use of the override feature when accessing medications in automated dispensing cabinets (ADCs).
The survey was initially scheduled to end on April 17, 2020. However, the window of opportunity to participate was extended until July 17, 2020, because many US hospitals were operating at full capacity and above during the early stages of the coronavirus (COVID-19) pandemic. While the overall response to this survey is less than with past ISMP surveys, and any delay in implementation of the new Best Practices is understandable during the pandemic, we want to sincerely thank the hospitals that participated in the survey and share the valuable lessons learned from the findings. An overview of the survey findings is presented in Table 1 and detailed below.
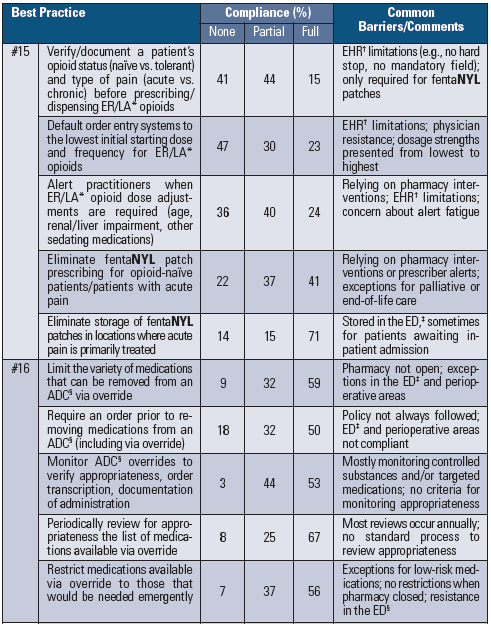
Table 1. Compliance with two new 2020-2021 ISMP Targeted Medication Safety Best Practices for Hospitals
Respondent Profile
Almost 250 (N = 247) US hospitals participated in our survey. More than a quarter (28%) of the responding hospitals were licensed for 500 beds or more; 18% had 300-499 beds; 27% had 100-299 beds; and 27% were smaller hospitals with 26-99 beds (15%) or 25 beds or less (12%). Overall, more than half (58%) of the hospitals reported employing one or more part- or full-time medication safety officer(s). The percentage of responding hospitals with a medication safety officer rose steadily as bed size increased, ranging from 25% in smaller hospitals with less than 100 beds to 85% in larger hospitals with 500 beds or more. With few exceptions, hospitals with a medication safety officer tended to report higher levels of implementation of the two new Best Practices. There were also differences in reported implementation levels based on bed size, as described below.
New Best Practice #15: Safe Opioid Prescribing
New Best Practice #15 comprises five interventions designed to improve safe prescribing of ER and LA opioids. The first intervention recommends verifying and documenting the patient’s opioid status (naïve versus tolerant) and type of pain (acute versus chronic) before prescribing and dispensing ER or LA opioids. Only 15% of hospitals reported full implementation of this intervention; 44% reported partial compliance; and 41% reported no implementation. Full implementation was greatest in hospitals with 26-99 beds (31%). Most reported barriers to implementation focused on limitations in the electronic health record (EHR), such as the inability to add a hard stop, alert, or mandatory field for the documentation of opioid status. Some respondents noted that documentation of opioid status is only required for certain opioids such as fentaNYL patches, patient-controlled analgesia (PCA), or large doses of ER and LA opioids. Many reported relying on pharmacists to evaluate the patient’s opioid status during order verification.
The next intervention recommends defaulting order entry systems to the lowest initial starting dose and frequency when initiating orders for ER and LA opioids. Less than one-quarter (23%) of hospitals reported full implementation; 30% reported partial compliance; and almost half (47%) reported no implementation. Full implementation was greatest in hospitals with 26-99 beds (27%). The most prevalent barrier reported was EHR limitations, and many respondents noted that their EHR currently presents all opioid dosage strengths from lowest to highest. Some hospitals reported physician resistance, while others reported defaulting to zero or the most commonly prescribed dose (which may not be the lowest starting dose). A few respondents reported low compliance with using opioid order sets or templates, nullifying the error-reduction impact of embedded dosing defaults.
The third intervention recommends alerting practitioners when ER and LA opioid dose adjustments are required due to age, renal or liver impairment, or when patients are prescribed other sedating medications. Less than one-quarter (24%) of hospitals reported full implementation; 40% reported partial compliance; and more than one-third (36%) reported no implementation. Smaller hospitals tended to report full implementation of this intervention more frequently than larger hospitals. Most respondents who have not implemented this intervention rely on pharmacists to intervene with dose adjustments during order verification. Respondents who reported partial compliance noted that drug-drug interaction alerts (for concomitant sedating agents) were more common, and renal or hepatic dosing alerts were least common. A few respondents expressed concerns about alert fatigue, overridden alerts, and EHR limitations with creating these alerts.
The fourth intervention recommends eliminating the prescribing of fentaNYL patches for opioid-naïve patients and/or patients with acute pain. Forty-one percent of hospitals reported full implementation of this intervention; 37% reported partial compliance; and almost one-quarter (22%) reported no implementation. Full implementation was greatest in hospitals with 300 beds or more (53%). Among hospitals that have not implemented this intervention, more than half reported they were either depending on alerts to warn prescribers about inappropriate prescribing or depending on pharmacists to intervene during verification. Several respondents reported that pharmacists have difficulty determining the appropriateness of fentaNYL patches because the patient’s opioid status is not known or documented, and that prescribers are sometimes confused regarding the criteria to determine opioid tolerance. A few respondents reported exceptions for palliative and end-of-life care.
The last intervention with Best Practice #15 recommends eliminating the storage of fentaNYL patches in ADCs or as unit stock in clinical locations where acute pain is primarily treated (e.g., emergency departments [EDs], operating rooms, post-anesthesia care units, procedural areas). Almost three-quarters (71%) of hospitals reported full compliance with this intervention; 15% reported partial compliance; and 14% reported no compliance with this intervention. Few barriers to implementation were reported, and those with partial compliance mostly reported that the patches remained in stock in the ED, sometimes for patients who were awaiting inpatient admission.
New Best Practice #16: Minimizing Use of the ADC Override Feature
New Best Practice #16 comprises five interventions designed to minimize the use of the override feature when accessing medications in ADCs. “Override” refers to the process of bypassing the pharmacist’s review of a medication order to obtain a medication from the ADC when assessment of the patient indicates that a delay in therapy would harm the patient. The first intervention recommends limiting the variety of medications that can be removed from an ADC using the override function. More than half (59%) of hospitals reported full implementation; 32% reported partial compliance; and 9% reported no compliance with this intervention. Full implementation was greatest in hospitals with 100 or more beds (66%). Among respondents reporting partial implementation, the most common barrier was that the pharmacy was not open 24 hours and did not employ remote order entry verification (requiring override access to medications in the ADC). Hospitals also reported specific locations, such as the ED and perioperative areas, where overrides occurred frequently. Most respondents who reported partial implementation felt their list of medications available via override could easily be pared down.
The next intervention recommends requiring a medication order (e.g., electronic, written, telephone, verbal) prior to removing any medication from an ADC, including those removed via override. Half (50%) of hospitals reported full compliance with this intervention; 32% reported partial compliance; and 18% reported no implementation of this intervention. Full implementation was greatest in hospitals with 100-499 beds (61%). Respondents reporting partial compliance frequently noted the presence of a policy that required an order prior to ADC removal of medications but said the policy is not always followed. Barriers to implementation included cultural issues and misperceptions that the removal of medications from an ADC alone serves as orders in perioperative and procedural areas. Several hospitals that reported full compliance told us that retrieving a medication from an ADC via override without an order is considered a medication error.
The third intervention recommends monitoring overrides to verify appropriateness, transcription of orders, and documentation of administration. Approximately half (53%) of hospitals reported full implementation; 44% reported partial compliance; and 3% reported no compliance. Full implementation was greatest in hospitals with 26-99 beds (92%). Hospitals reporting partial compliance said they are monitoring overrides only for controlled substances or other targeted or randomly selected medications due to time constraints. Some respondents also noted that overrides are only reviewed for a corresponding order and documentation of administration, not the appropriateness of the override.
The fourth intervention recommends periodically reviewing for appropriateness the list of medications available using the override function. Two-thirds (67%) of hospitals reported full compliance with this intervention; 25% reported partial compliance; and 8% reported no compliance. Few barriers were reported, and most respondents reporting full compliance said they reviewed lists annually.
The last intervention recommends restricting medications available via override to those that would be needed emergently (organization-defined) such as antidotes, rescue/reversal agents, life-sustaining drugs, and comfort measure medications (e.g., for acute pain, intractable nausea/vomiting). More than half (56%) of hospitals reported full compliance with this intervention; 37% reported partial compliance; and 7% reported no compliance. Full implementation was greatest in hospitals with 100 or more beds (61%). Respondents who reported partial compliance noted that additional access to medications in ADCs was required when the pharmacy was closed. A few respondents reported resistance to limiting access in certain locations, including the ED. Several respondents told us about low-risk medications that had been made available via override to facilitate throughput in the ED and perioperative locations.
Conclusion
These survey results suggest there is sizeable room for improvement during 2020-2021 with the two new Best Practices associated with safe opioid prescribing and minimizing ADC overrides. We hope that hospitals will take note of the barriers and misperceptions that may delay implementation of these important safety strategies, and use the survey results to prompt interdisciplinary discussions about potential barriers to implementation along with brainstorming ways to resolve them.
For example, a discussion about Best Practice #15 might lead to the discovery of the best process to collect and document the opioid status of patients. Some providers ask all new patients about opioid use (including heroin and/or non-prescribed opioids) during the past few weeks and make an initial determination of opioid status when creating a home medication list, which is verified upon medication reconciliation and documented on the patient’s medication list or in the EHR. Other providers require a determination of opioid status per established criteria with all opioid pain management order sets, which guide the selection and dosing of opioids. An interdisciplinary discussion about Best Practice #16 might lead to a requirement to document the rationale for any overrides, ADC screen changes to facilitate this process, the development of criteria to monitor the appropriateness of all ADC overrides, the adoption of remote pharmacy order verification when the pharmacy is closed, the use of profiled ADCs in all clinical areas, and the commission of an interdisciplinary group to routinely analyze all (not just controlled substances) override reports to identify if an order was obtained prior to removing the medication and whether the rationale for each overridden medication was appropriate.
The basis for recommending the two new Best Practices, along with related ISMP publications and guidelines for additional information, can be found in the full 2020-2021 ISMP Targeted Medication Safety Best Practices for Hospitals. An Implementation Worksheet for all of the Best Practices is also available and might be helpful.
Access this Free Resource
You must be logged in to view and download this document.