
Implement strategies to prevent persistent medication errors and hazards
Reflecting on events of 2022, we have identified the top medication errors and hazards that were themes in the ISMP Medication Safety Alert! which can also be found in ECRI’s Top 10 Patient Safety Concerns for 2023. Our selected top concerns are not solely based on the most frequently reported problems or those that have led to the most serious consequences for patients, although these factors were considered. Rather, we focused on errors and hazards that continue to occur but can be avoided or minimized with system and/or practice changes. If you have not already taken action to mitigate these risks, we believe these issues are important enough to warrant attention and priority in the coming year. Links to additional related content in our newsletters and guidelines are provided along with the descriptions below (some links require you to sign into the ISMP website for access). We hope that awareness about these important errors and hazards informs priorities in your 2023 medication safety improvement plan!
Overreliance on Holding Practitioners Accountable for the Five Rights
"The Five Rights” are broadly stated expectations set forth with the desire to achieve safe medication practices. The belief is that the five rights will ensure the right patient is given the right medication, at the right dose, at the right time, and via the right route. However, the five rights must be recognized for what they are, merely desired outcomes for safe medication practices. In an attempt to reach the desired outcome, some organizations require more than five rights, which still do not address system problems. Unfortunately, they are continually exploited to perpetuate the mistaken belief that healthcare professionals, particularly frontline nurses, can be held individually accountable for achieving those standards within the flawed healthcare delivery systems they often practice. Weaknesses associated with this erroneous guidance include the following:
-
The five (six, seven, eight, nine, ten, etc.) rights (aka “rules") do not provide procedural guidance on how to achieve the desired outcome.
-
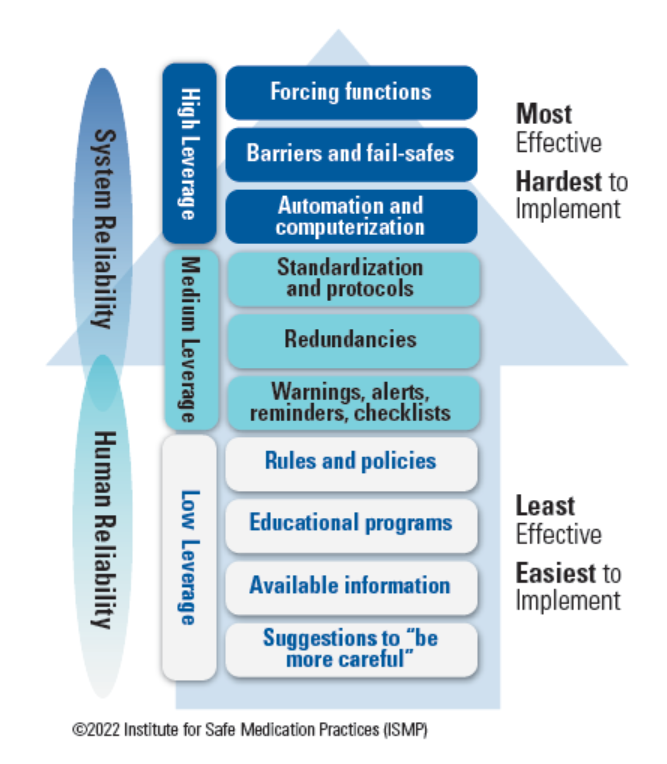
Instructing a healthcare practitioner to follow the five rights is a low-leverage strategy in ISMP’s Hierarchy of Effectiveness of Risk-Reduction Strategies (Figure 1), one that relies solely on the performance of an inherently fallible human being at the sharp end of the medication-use process.
-
Many errors, including lethal errors, have occurred in situations where practitioners believed they had verified the five rights.
-
The responsibility for accurate medication administration does not lie with a single individual. Rather, it lies with multiple individuals, including organizational leaders, who are responsible for the design, implementation, and maintenance of reliable systems to support safe medication use for all practitioners.
-
A medication-use system that is inadequate or poorly designed to support practitioners will lead to errors.
-
Human factors play a significant role in the occurrence of errors, a fact that the focus on the five rights ignores.
-
Emphasizing the five rights during the review of medication errors may blind the reviewer to latent failures that exist within the system that should be the focus of the investigation.
Recommendations: The healthcare industry needs to stop perpetuating the belief and expectation that practitioners can and should be held individually accountable for the performance of medication-use systems by achieving “compliance” with the five rights. Ultimately, prevention of medication errors relies on the integrity of several complex, interrelated systems designed with high-leverage safety practices and strategies to reduce risks and limit harm, coupled with clearly defined processes and behavioral expectations. An interdisciplinary team of healthcare professionals and organizational leaders must work collaboratively to implement these systems and to coach safe behaviors in support of safe systems. These systems should also be actively managed and continually monitored, not only to measure their effectiveness, but more importantly to make changes and improvements as necessary.
Medication Errors Resulting from Inaccurate Patient Medication Lists
Lack of, or miscommunication about, prescribed and discontinued medications occurs commonly during vulnerable transition points in the continuum of care (e.g., hospital admission, transfers between care settings, discharge). If a patient’s medication list is not accurate, it can result in the patient receiving an incorrect medication or dose, receiving a medication too soon or too late if the time of their last dose is inaccurate, receiving inappropriate or duplicate therapies, or the omission of a critical medication. According to the Institute for Healthcare Improvement (IHI), experience from several organizations has shown that poor communication of medical information at transition points is responsible for as many as 50% of all medication errors and up to 20% of adverse drug events in hospitals. This is precisely why The Joint Commission (TJC) has focused attention on reducing the risk of errors during transitions of care through the use of the medication reconciliation process (NPSG.03.06.01).
Recommendations: Educate staff and dedicate resources to facilitate accurate medication reconciliation. Multidisciplinary medication reconciliation teams should review current processes, identify gaps and opportunities for improvement, and lead process design and redesign within the organization by implementing the following recommendations:
Admission
-
Have practitioners approach admission medication reconciliation as a three-step process:
-
Verify. Obtain the most accurate medication list possible (See ISMP Canada’s Best Possible Medication History [BPMH]) upon admission to the organization before the first dose of medication is administered (except in emergency or urgent situations). Incorporate prompts in the electronic health record (EHR) for staff to ask about allergies, prescription and over-the-counter medications (including herbals and dietary supplements) and non-enteral medications (e.g., patches, eye and ear drops, topical and inhaled medications, injectables and infusions). List the drug name, dose, route, frequency (including time of administration), indication, and time of the last dose. Sources of information may include visual inspection of the medications brought into the facility by the patient or family, previous medical records, the patient's pharmacy and prescriber’s office, or online prescription data. Verify this information with the patient or their family/caregiver to validate an accurate list of current medications as well as the patient’s compliance with their medication regimen.
-
Clarify. After documenting the patient’s medication list in the EHR, ensure the medication and doses collected and subsequently ordered are the correct therapy for that patient, given that patient’s current state of health, or seek clarification.
-
Reconcile. Designate a provider to compare the prescribed admission medications to those on the medication history list and resolve any discrepancies. Document any modifications made to the current therapy upon admission, with each change in the level of care, and at discharge to promote a continuum of safe medication use.
-
Transfer
-
Each time a patient transfers from one level of care or setting to another (e.g., critical care to medical/surgical, operating room to medical/surgical), review previous medication orders alongside new and discontinued orders and the plan of care and resolve any discrepancies.
Discharge
-
Prior to discharge, designate a provider to reconcile the patient’s list of admission medications against the discharge orders along with the most recent medication administration record (MAR). Any differences must be resolved before discharge.
-
Provide the patient with an updated medication list and communicate which medications they are to continue taking, those they should stop taking, and any new medications for them to start taking. Educate patients on each medication’s indication, how they should take it, and common side effects.
-
Send a complete list of the patient's medications to the next service provider when discharging the patient or transferring the patient to another level of care within the organization to another care setting outside the facility. Even if the patient is going home, send the list directly to the patient’s primary care provider (PCP), if possible.
-
Educate patients on the importance of maintaining and carrying a complete and up-to-date medication list. Encourage patients to share the list during all healthcare encounters (e.g., prescriber’s office, pharmacies, hospitalizations).
Accidental Administration of Neuromuscular Blocking Agents
Neuromuscular blocking agents paralyze skeletal muscles and are considered high-alert medications as they are known to cause catastrophic injuries or death when used in error. Over the last 25 years, ISMP has received more than 100 reports concerning accidental neuromuscular blocking agent administration. Inadequate labeling or unsafe storage has been a root cause of most of these errors. Since 2016, our Targeted Medication Safety Best Practices for Hospitals, Best Practice #7, has called for organizations to segregate, sequester, and differentiate all neuromuscular blocking agents from other medications, wherever they are stored in the organization. Despite the well known risk of mix-ups, errors involving neuromuscular blocking agents continue to occur throughout the medication-use process.
Recommendations: In alignment with Best Practice #7, restricting access, segregating storage areas, and the use of proper warning labels can be used together as effective means of preventing mix-ups with neuromuscular blocking agents. Start by reviewing our previous publications (Paralyzed by Mistakes - Reassess the Safety of Neuromuscular Blockers in Your Facility, Safety Enhancements Every Hospital Must Consider in Wake of Another Tragic Neuromuscular Blocker Event, and Criminalization of Human Error and a Guilty Verdict: A Travesty of Justice that Threatens Patient Safety) to reassess risk in your organization and implement the following safeguards:
-
Eliminate the storage of neuromuscular blocking agents in areas of your organization where they are not routinely needed.
-
Segregate neuromuscular blocking agents from all other medications in the pharmacy by placing them in separate lidded containers in the refrigerator or other secure, isolated storage areas.
-
Limit availability in automated dispensing cabinets (ADCs) to areas where they are needed such as perioperative, labor and delivery, critical care, and emergency department (ED) settings; in these areas, store them in a rapid sequence intubation (RSI) kit, or locked-lidded ADC pockets/drawers.
-
Place auxiliary labels on all storage bins (both refrigerated and non-refrigerated) and/or ADC pockets and drawers that contain neuromuscular blocking agents. Also, label all final medication containers (e.g., syringes, intravenous [IV] bags) that state: “WARNING: CAUSES RESPIRATORY ARREST – PATIENT MUST BE VENTILATED” or “WARNING: PARALYZING AGENT – CAUSES RESPIRATORY ARREST” or “WARNING: CAUSES RESPIRATORY PARALYSIS – PATIENT MUST BE VENTILATED” to clearly communicate that respiratory paralysis will occur and ventilation support is required.
-
Configure interactive ADC alerts that require users to enter or select clinically relevant information (e.g., the purpose for removing the drug [a code situation], whether the patient is ventilated) prior to removal.
-
Implement pharmacy IV workflow management systems and require barcode scanning of each ingredient for positive identification before it is introduced in the compounding process. These systems should not only be used for high-alert medications (e.g., neuromuscular blocking agent infusions) but for all medications, as sometimes high-alert medications are inadvertently selected instead of a non-high-alert medication during the compounding process.
Suggested citation:
Institute for Safe Medication Practices (ISMP). Implement strategies to prevent persistent medication errors and hazards. ISMP Medication Safety Alert! Acute Care. 2023;28(6):1-4.
Access this Free Resource
You must be logged in to view and download this document.