
Medical Abbreviations That Have Contradictory or Ambiguous Meanings
ISMP would like to thank Neil M. Davis, PharmD, MS, FASHP, for authoring this article. The author can be reached at: [email protected] for any comments or questions.
Introduction
Abbreviations are a convenience, a time saver, and a way of fitting a word or phrase into a restricted space or avoiding the possibility of misspelling words. However, a high price can be paid for their use. Abbreviations are sometimes not understood, misread, or interpreted incorrectly. Their use lengthens the time needed to train healthcare professionals; wastes time tracking down their meaning; sometimes delays the patient’s care; and occasionally results in patient harm.
I published my first book of medical abbreviations, Medical Abbreviations: 1,700 Conveniences at the Expense of Communication and Safety, in 1983. To expand the list of abbreviations, I contacted hospitals and requested lists of abbreviations that were used at their facility, searched the literature, and solicited readers to send me abbreviations. Since then, I have published 16 editions of the book, which now contains 55,000 abbreviations.1 A web version of the book is updated with more than 30 new entries per week.2
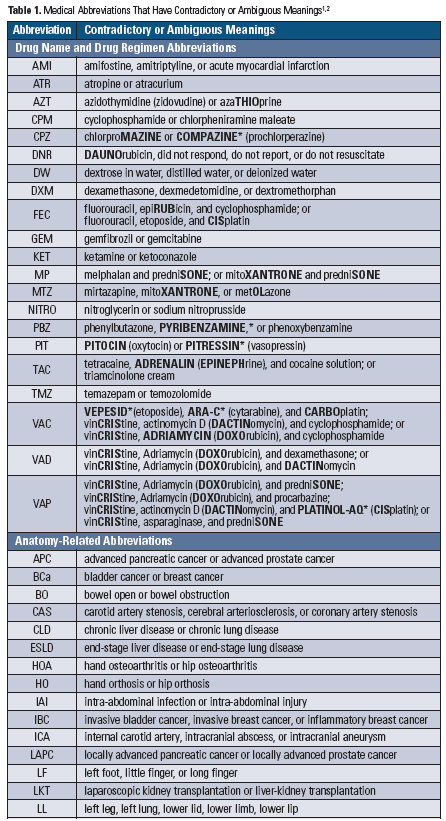
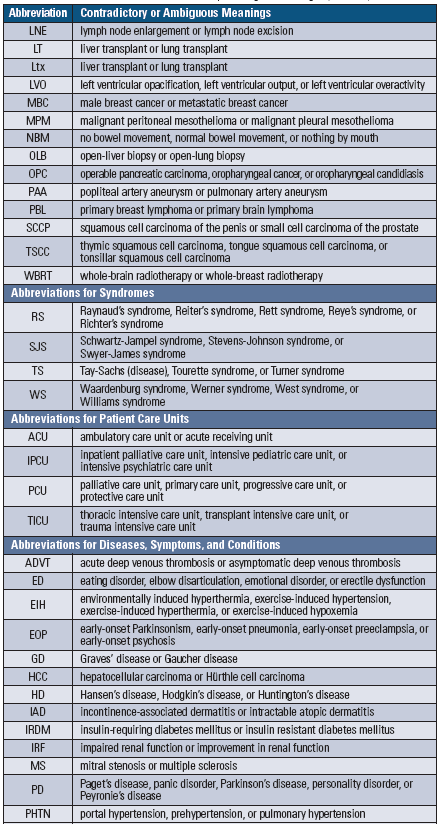
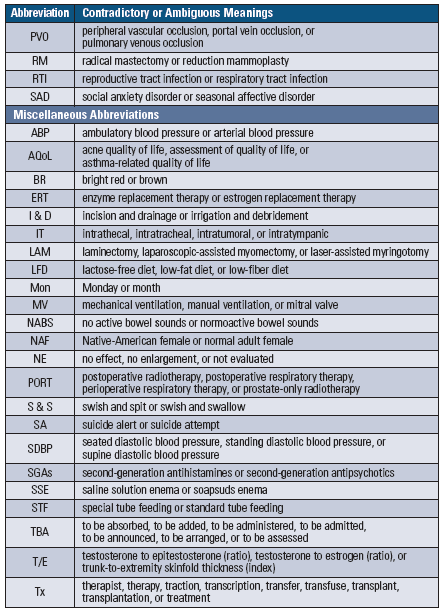
One of the problems I noticed was that one abbreviation could have two or more contradictory or ambiguous meanings, which can create dangerous communications. I collected these meanings, and a partial list of medical abbreviations with contradictory or ambiguous meanings is shown in Table 1 (below). It is obvious from an examination of this list that these abbreviations should not be used, as they fail to communicate with any certainty their intended meaning and present possible dangers to the health of patients.
The Joint Commission directs medical facilities to publish a Do Not Use List3 of abbreviations that must not be used (see ISMP’s list). This list is a very important step in the right direction but does not solve the systemic problem of an abbreviation with contradictory or ambiguous meanings.3 The Joint Commission standards also state, if multiple abbreviations exist for the same term, the organization must identify which one will be used to eliminate ambiguity.4 This step is extremely difficult to achieve.
Two Possible Solutions That May Not Be Feasible
1. Create a national list of standard abbreviations. A simplistic approach to this problem is to create a national list of approved abbreviations, with each abbreviation having only one meaning. The problem with this approach is that all medical specialties, allied health professionals, health-related organizations, and government agencies would have to agree on one meaning for each abbreviation.
A recognized health-related organization, such as USP, the American Medical Association, the Council of Science Editors, ISMP, or ECRI Institute, would have to be funded to take responsibility for creating and maintaining such a list. The organization would have to reach out to all the health-related organizations to suggest abbreviations that should be on this list. Then, arbitration would be required between organizations if there is conflict with a suggested abbreviation that has more than one submitted meaning, such as PT for physical therapy, prothrombin time, preterm, parathyroid, patellar tendon, patient, and others. Such an endeavor would take hundreds of thousands of hours. Furthermore, after an approved list is created, it must be maintained. Any new abbreviations would require review and approval by all interested parties. Also, there could be a troublesome lapse of time before a new proposed medical abbreviation is commonly known and used—MRI for magnetic resonance imaging is an example of such a situation.
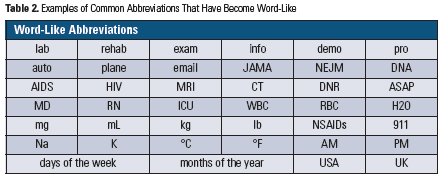
2. Not allowing abbreviations. Not allowing the use of any abbreviations would be an exceedingly difficult edict to introduce and enforce. Practitioners have used abbreviations in their daily routine, and it would be difficult to break this habit. In fact, some abbreviations that are frequently used have become word-like, making it especially challenging to require use of the full words instead. Examples are listed in Table 2 (below).
Since it is highly unlikely that abbreviations will ever be eliminated, and naïve to assume that they can be systematically approached in any realistic timeframe, the healthcare professions must work together to insure that abbreviations are used appropriately.
What Healthcare Practitioners, Agencies, Authors, and Editors Can Do
Before practitioners, researchers, and authors introduce a new abbreviation, they must question whether it is necessary to do so. Do not create an abbreviation that is already in use for some other meaning or has a contradictory or ambiguous meaning. To accomplish this, use comprehensive and up-to-date resources such as the US National Library of Medicine’s PubMed, web search engines, medical abbreviations books, and websites.
There are several character similarities and risky abbreviation construction practices that are apparent in Table 1 (below), which should serve as a signal that many medical abbreviations can be easily misinterpreted and may be dangerous. These characteristics should lead to the following guiding principles when it comes to medical abbreviations:
-
Avoid abbreviating drug names entirely
-
Employ great care when abbreviating health syndromes, diseases, and conditions
-
Be particularly sensitive to the problems caused by the following abbreviations:
-
B for breast, brain, or bladder
-
C for cerebral, coronary, or carotid
-
H for hand or hip
-
I for impaired or improvement
-
L for liver or lung
-
N for no or normal
-
P for pancreas, prostate, preeclampsia, or psychosis
-
S for special or standard
-
Authors and medical editors must follow these principles when reviewing and editing proposed manuscripts to make sure they do not introduce contradictory, ambiguous, or dangerous abbreviations into the health-related vocabulary. No abbreviation should be used in titles and abstracts unless it is defined, as the body of the text will not appear in an abstracting service. Any abbreviations used in the body of the text must be defined.
The person who uses an abbreviation must take responsibility for making sure that it is properly interpreted. When an uncommon or ambiguous abbreviation is used and it may not be understood correctly, it should be defined by the writer/sender (even on professional discussion boards). Where uncertainty exists, clarification with the one who used the abbreviation is required. There is hope that IBM Watson-like products, artificial intelligence, and future technologies can be used to devise additional workable solutions.
References
- Davis NM. Medical Abbreviations: 55,000 Conveniences at the Expense of Communication and Safety. 16th ed. Warminster, PA: Neil M. Davis Associates; 2020.
- MedAbbrev.com. Website by Neil M. Davis; 2020.
- The Joint Commission. Medication errors related to potentially dangerous abbreviations. Sentinel Event Alert. 2001;Sep(23):1-4.
- The Joint Commission. Information management standard IM.02.02.01, EP 2, 3. 2020 Comprehensive Accreditation Manual for Hospitals (CAMH). Oakbrook Terrace, IL: The Joint Commission; 2019.
©MedAbbrev.com.2 Table may be reproduced/republished with permission only.
Access this Free Resource
You must be logged in to view and download this document.